
Dear Church Leaders (and everyone else)
Six months ago, in this article…

…I wrote that:
I am now inclined to ask basic questions about the truthfulness of any unusually high-profile media story that has at least some of the following features:
Strong emotions are evoked
There is widespread mainstream media coverage…
And with that in mind I thought it worth sharing some thoughts and information in relation to what this UK government website describes as:
…an evolving situation involving multiple cases of invasive meningococcal disease (IMD) reported among young people linked to the University of Kent and the Canterbury area.
This particularly Canterbury tale has certainly had widespread mainstream media coverage. For example, here are the results of a BBC News search for “meningitis” at the time of writing (7pm, Thursday 19th March):
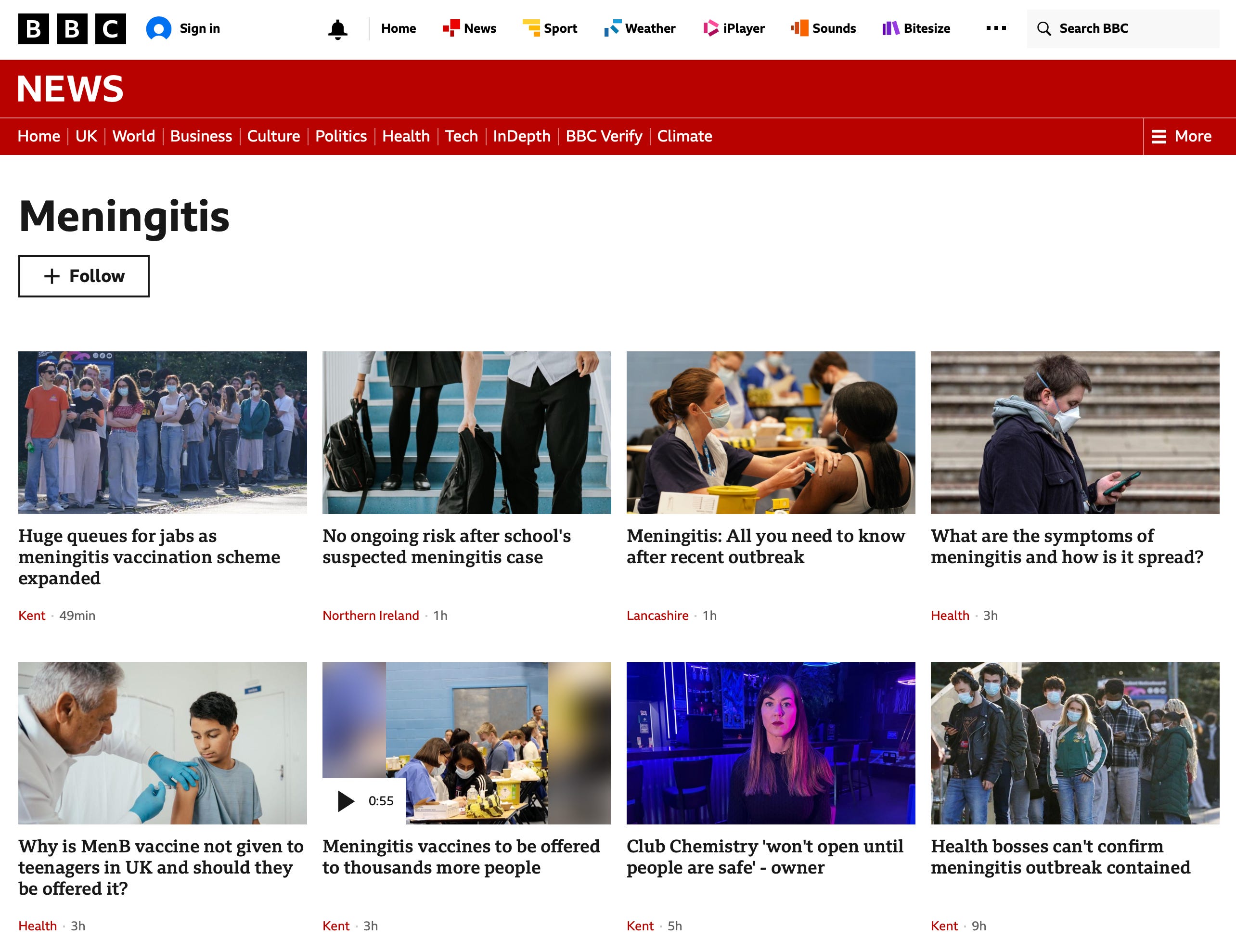
Those are the first eight of around fifty articles in two days or so from the same BBC which stated, in the context of their lack of coverage of the Rape Gang Inquiry backed by Rupert Lowe, that “We have limited resources and it is not possible to report on every story which is of interest to our audiences.”
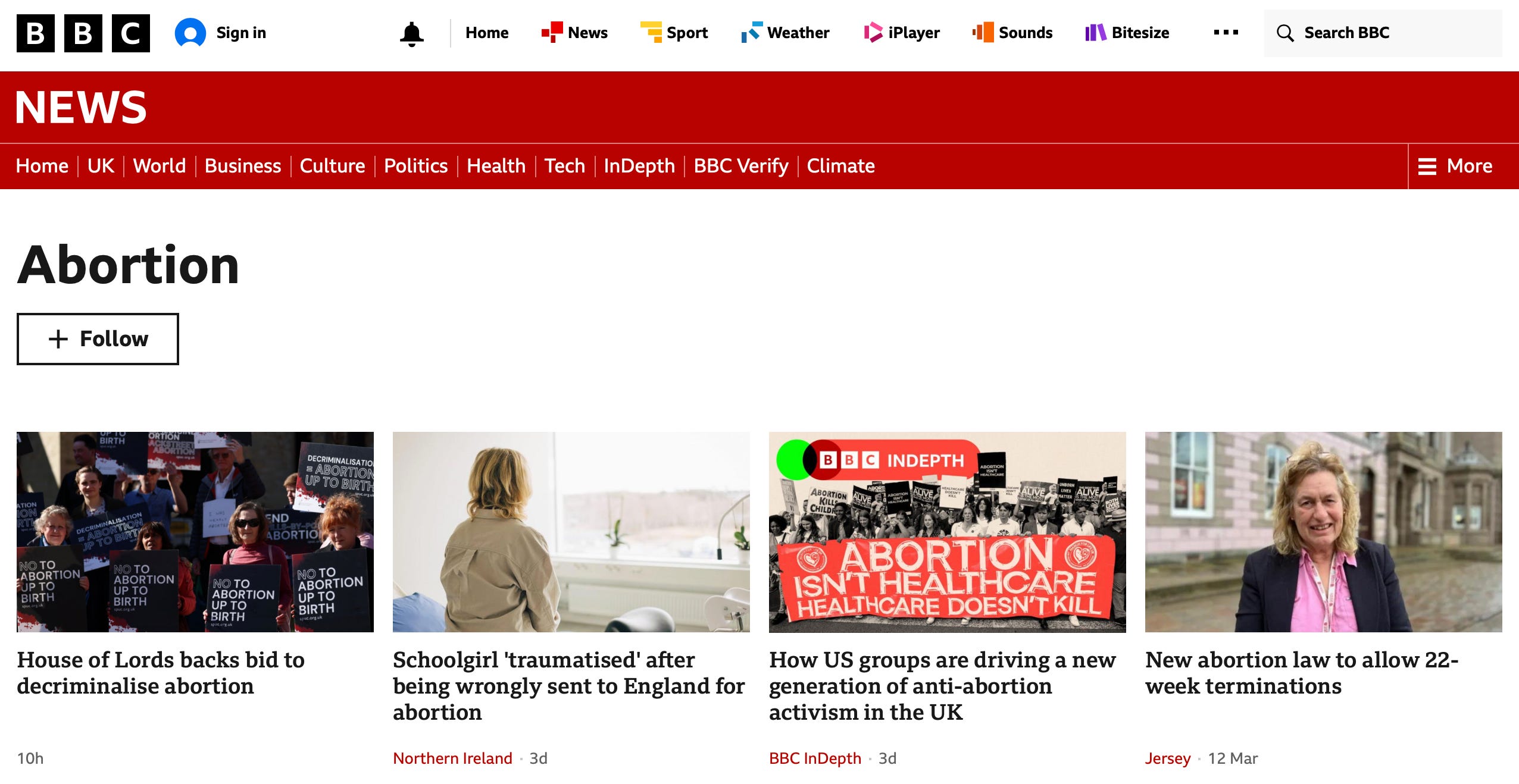
In contrast, here are the results for a search for “abortion” (in the context of Wednesday’s House of Lords vote backing the decriminalisation of abortion up to birth):
In the spirit of “Watch out that you are not deceived”, and also Proverbs 18:17 and Ephesians 4:25, I offer some cautionary context below.
Prevalence
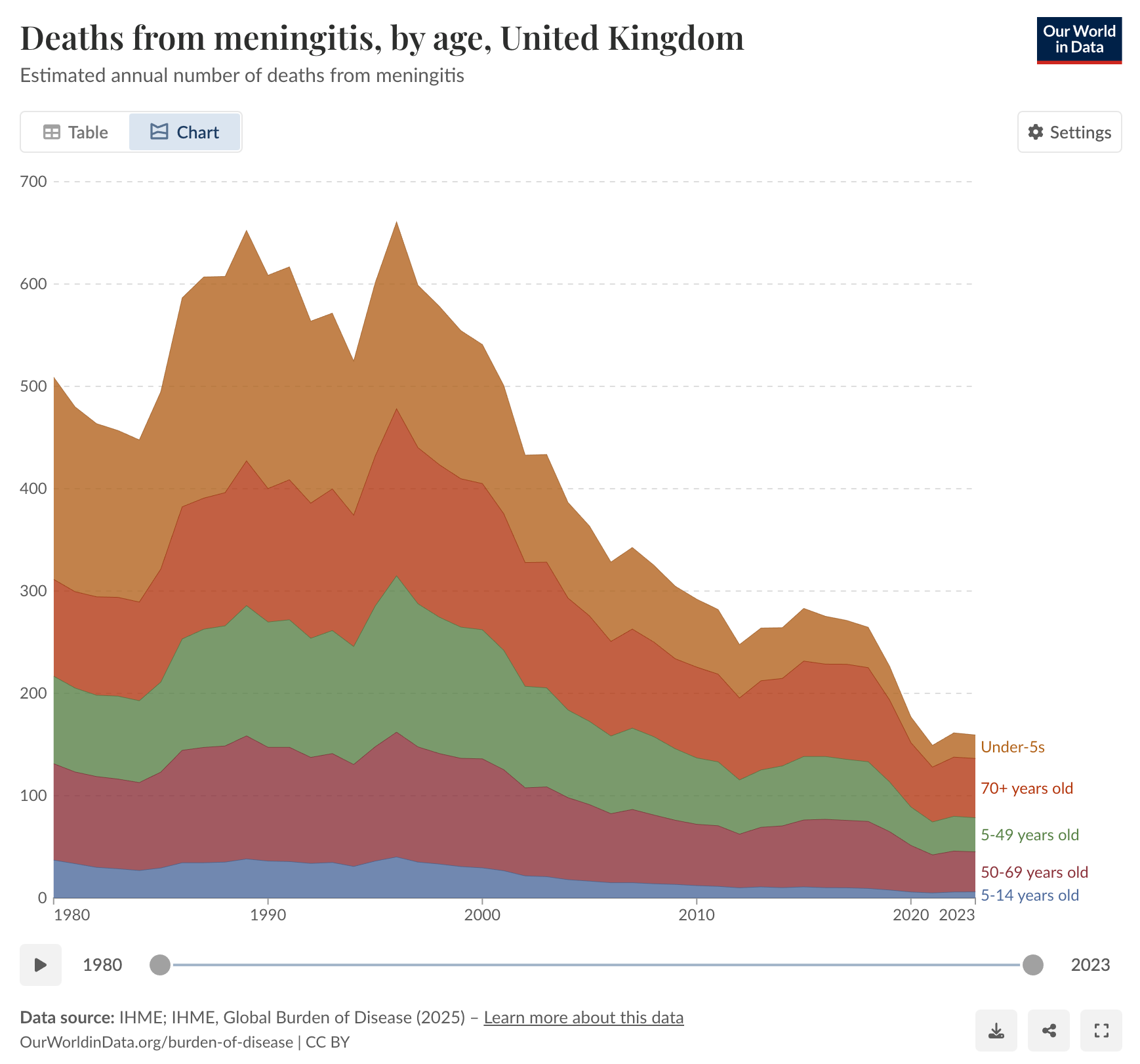
Here is a chart showing the estimated annual number of deaths from meningitis, by age, in the UK:
Prof Carl Heneghan (based at the University of Oxford Centre for Evidence-Based Medicine) and Dr Tom Jefferson (an epidemiologist based in Rome who works with Heneghan on the Cochrane Collaboration) recently shared this graph, breaking down the incidence per 100,000 into infants, teens and adults:
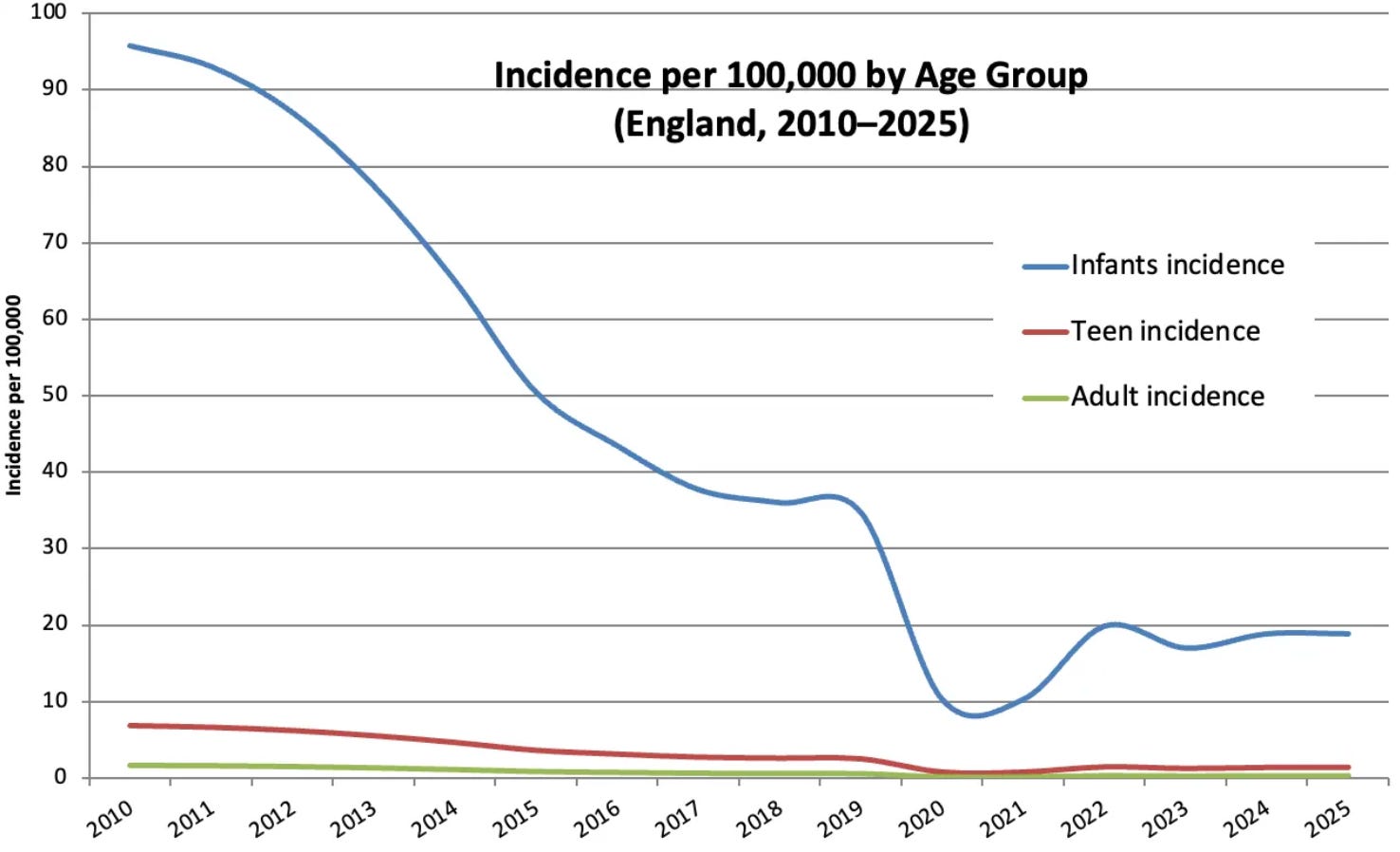
They comment (emphasis added):
Making some assumptions about the age distribution of the population, infants [as distinct from teens] have a roughly 15–60 times higher incidence than adults, who have a very low baseline risk.
Symptoms
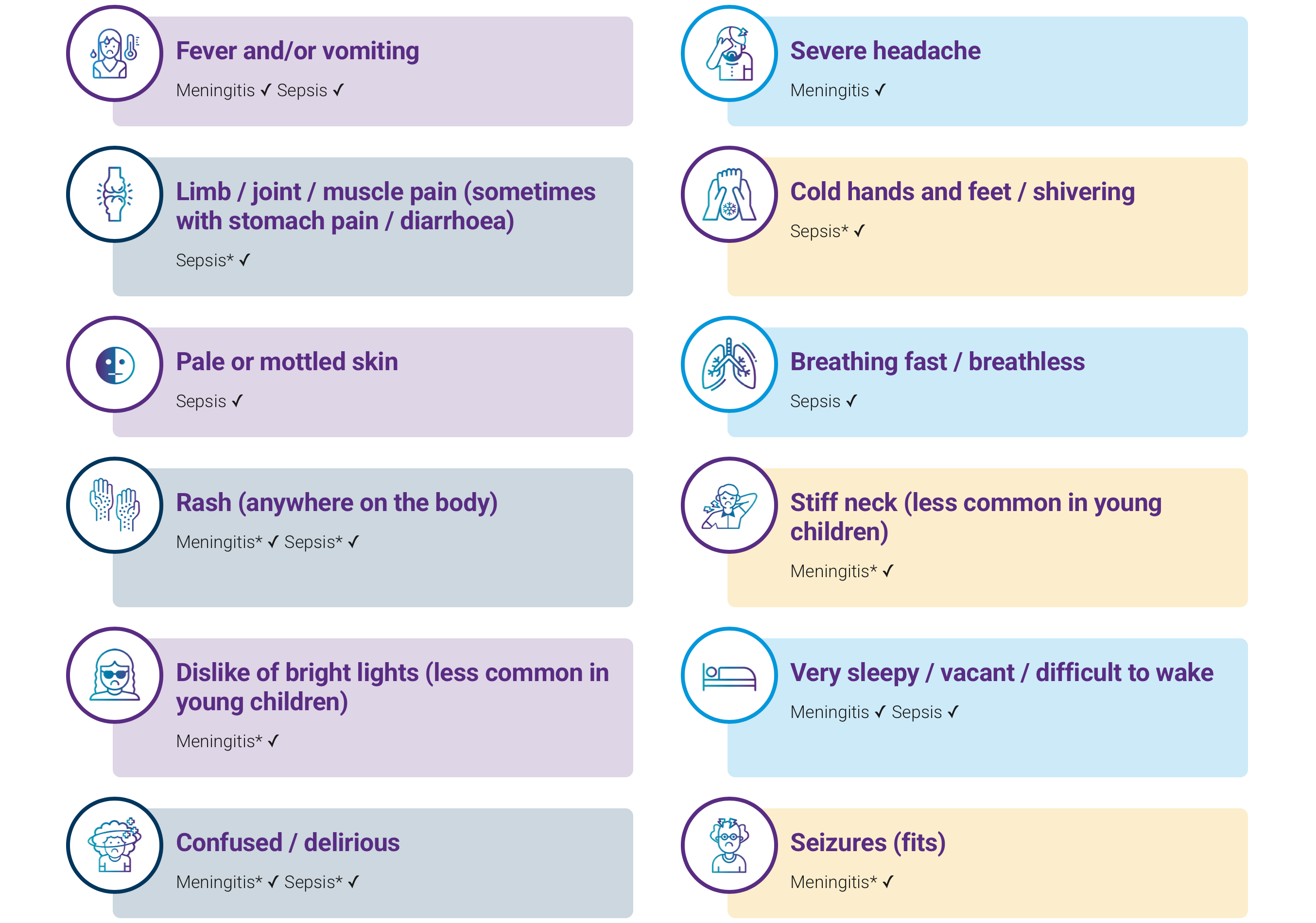
According to meningitis.org…
The first symptoms [of meningitis] are usually fever, vomiting, headache and feeling unwell…
…which does rather remind me of times of illness in my own life, perhaps more than once as a student. But I am all but certain that I have never had any form of meningitis.
Moreover, how different are the above symptoms from those that might be expected in someone who had stayed up into the small hours dancing the night away at Club Chemistry, and perhaps misjudged their intake of alcohol (to say nothing of any other substances)?
More broadly, I can’t help but think of a certain respiratory virus that led to something of a public health scare a few years back, two of whose main symptoms were a temperature and a persistent cough.
Diagnosis
In many areas of medicine there are quick and cheap tests that can provide a useful indicator but which can also give results that can be misleading. Indeed false positive test results can create the impression of an epidemic when, actually, there isn’t one.
Here is a real world example1 reported in The New York Times in 2007 under the headline Faith in Quick Tests Leads to Epidemic That Wasn’t (emphasis added):

For months, nearly everyone involved thought the medical center had had a huge whooping cough outbreak, with extensive ramifications. Nearly 1,000 health care workers at the hospital in Lebanon, N.H. [New Hampshire], were given a preliminary test and furloughed from work until their results were in; 142 people, including Dr. Herndon, were told they appeared to have the disease; and thousands were given antibiotics and a vaccine for protection. Hospital beds were taken out of commission, including some in intensive care.
Then, about eight months later, health care workers were dumbfounded to receive an e-mail message from the hospital administration informing them that the whole thing was a false alarm.
Which is not to deny that some of those people with a positive test were actually sick with something:
Not a single case of whooping cough was confirmed with the definitive test, growing the bacterium, Bordetella pertussis, in the laboratory. Instead, it appears the health care workers probably were afflicted with ordinary respiratory diseases like the common cold.
Quick and cheap tests are not usually the only tests available. But they are convenient, and profitable. In contrast, proper diagnosis, which often includes other testing and investigation, takes longer and costs more, especially if medical appointments are involved. But the outcome is much more likely to be accurate.
According to this UK government website:
PCR assays are used to detect N. meningitidis DNA… where possible.
PCR [polymerase chain reaction] assays were of course used to test for covid.
But it is important to remember that Kary Mullis, the Nobel prize-winning inventor of PCR, stated that:
PCR [polymerase chain reaction] is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing that you ended up with was going to hurt you or anything like that.
And that:
With PCR, if you do it well, you can find almost anything in anybody.
One of the ironies here is that testing an unprecedented number of healthy people can cause an unprecedented number of false positive “cases”. And the appearance of “an unprecedented outbreak”.
Moreover, PCR testing is open to manipulation. If the number of cycles is set high, the number of positive results is hight. If the number of cycles is reduced (perhaps after certain public health interventions), the number of positives results falls, giving “evidence” of the “success” of those interventions. It was in that context that I found the UK government’s October 2020 statement that “the United Kingdom operational false positive rate [for the PCR test] is unknown” more than a little concerning.
I guess that if Mullis were still alive, he would make the above points himself, which would carry a lot of weight coming from a Nobel laureate. Alas, as I discussed in this post, he died unexpectedly in 2019, a few months before the covid PCR testing started.
As to the proper diagnosis of meningitis, according to the UK’s National Institute for Health and Care Excellence (emphasis added):
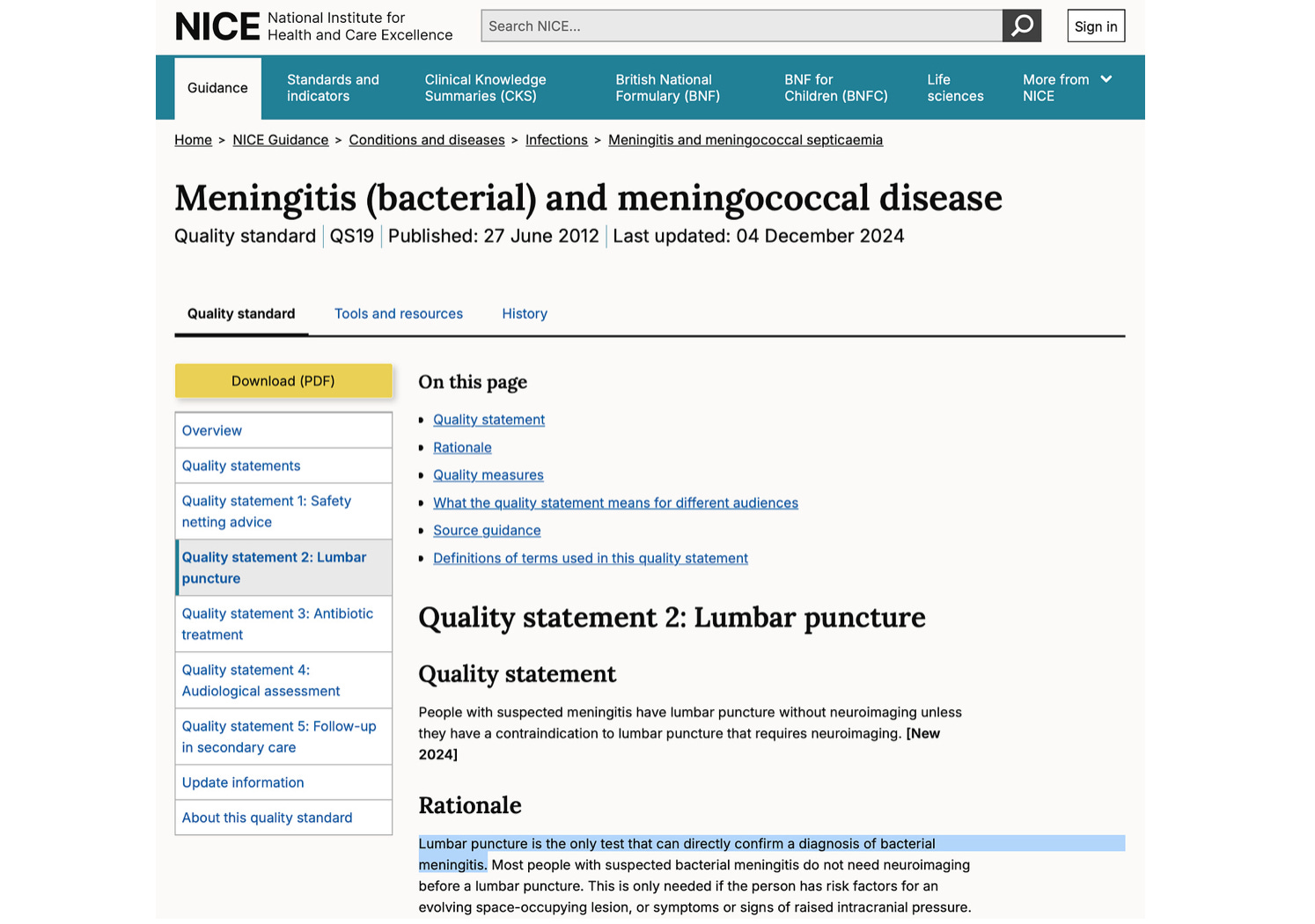
Lumbar puncture is the only test that can directly confirm a diagnosis of bacterial meningitis.
Lumbar puncture doesn’t exactly sound appealing though. I asked Alter AI:
Tell me about lumbar puncture and the advantages and disadvantages of it (80 words)
And I got this response:
A lumbar puncture, or spinal tap, involves inserting a needle into the lower spine to collect cerebrospinal fluid for analysis. It’s commonly used to diagnose meningitis, multiple sclerosis, and subarachnoid hemorrhage, or to administer medication.
Advantages: provides direct, precise neurological information, guides treatment, and sometimes relieves intracranial pressure.
Disadvantages: may cause headaches, discomfort, infection, bleeding, or nerve irritation.
Though generally safe when performed correctly, it must be used judiciously—only when diagnostic benefits clearly outweigh potential risks.
Ironically, as noted earlier, a headache is one of the first symptoms of meningitis.
But while NICE states that lumbar puncture is the only test that can directly confirm a diagnosis of bacterial meningitis, the government tells us that…
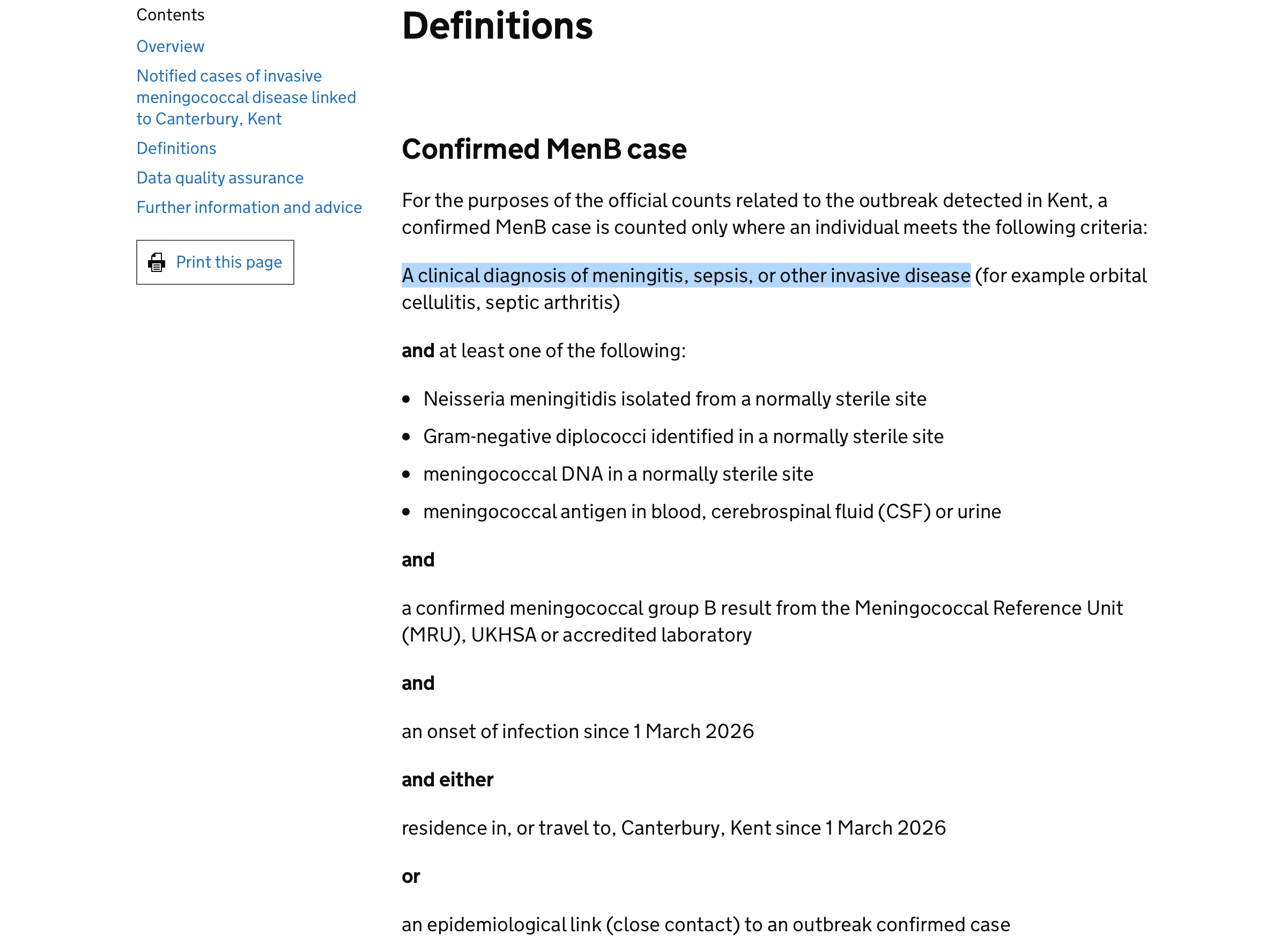
“For the purposes of the official counts related to the outbreak detected in Kent”, it seems it is not actually necessary to have a clinical diagnosis of meningitis.
In relation to the above, I asked AlterAI:
In the UK, how many people each year receive a clinical diagnosis of (1) meningitis, (2) sepsis; (3) another invasive disease (for example orbital cellulitis, septic arthritis) (50 words)
Here is the response:
Each year in the UK, around 8,000–10,000 people are diagnosed with meningitis, approximately 245,000 with sepsis, and an estimated 40,000–60,000 experience other invasive bacterial diseases such as orbital cellulitis or septic arthritis. Rates fluctuate annually depending on surveillance definitions, bacterial strain circulation, and underreporting within hospital diagnostic data systems.
Antibiotics
The UK government website cited earlier also states, under the somewhat verbose heading of “Providing antibiotic chemoprophylaxis”, that:
Close contacts of confirmed or probable cases are being identified by UKHSA and require antibiotic prophylaxis. Timely chemoprophylaxis will prevent cases of disease and will save lives. Antibiotic prophylaxis should be given as soon as possible (ideally within 24 hours) after the diagnosis of the index case, regardless of vaccination status.
It goes on to add that:
In response to this outbreak, a wider group of contacts have been identified as requiring antibiotic prophylaxis on a precautionary basis:
Students who live on the Canterbury campus at the University of Kent
Staff who live or work in affected halls of residence blocks on the Canterbury campus at the University of Kent
Staff members working at Club Chemistry nightclub, Canterbury, and anyone who attended the nightclub as visitors on 5, 6 or 7 of March 2026.
According to this NHS website dated 18th March…
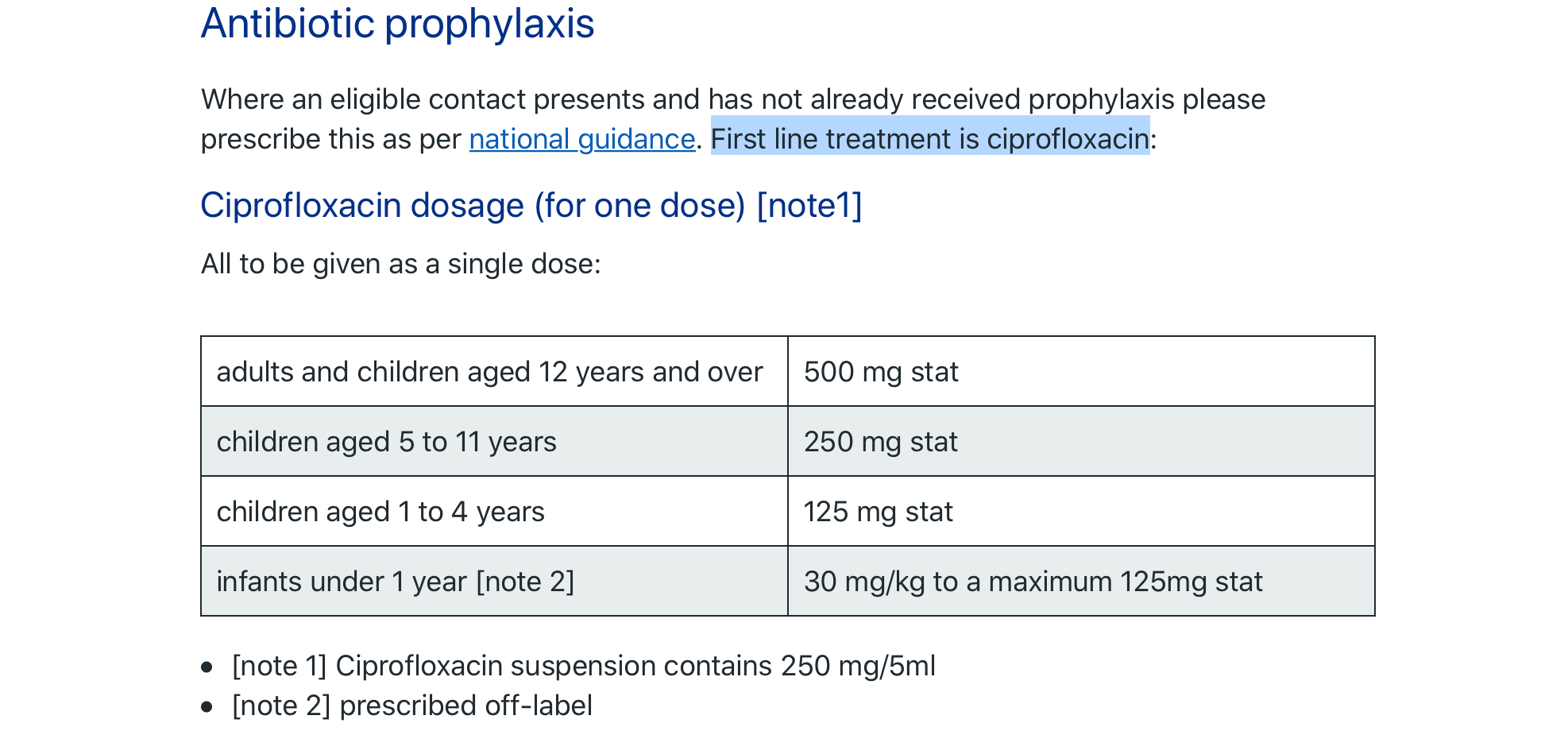
…the “first line treatment is ciprofloxacin”, which is consistent with page 3 of this advice…
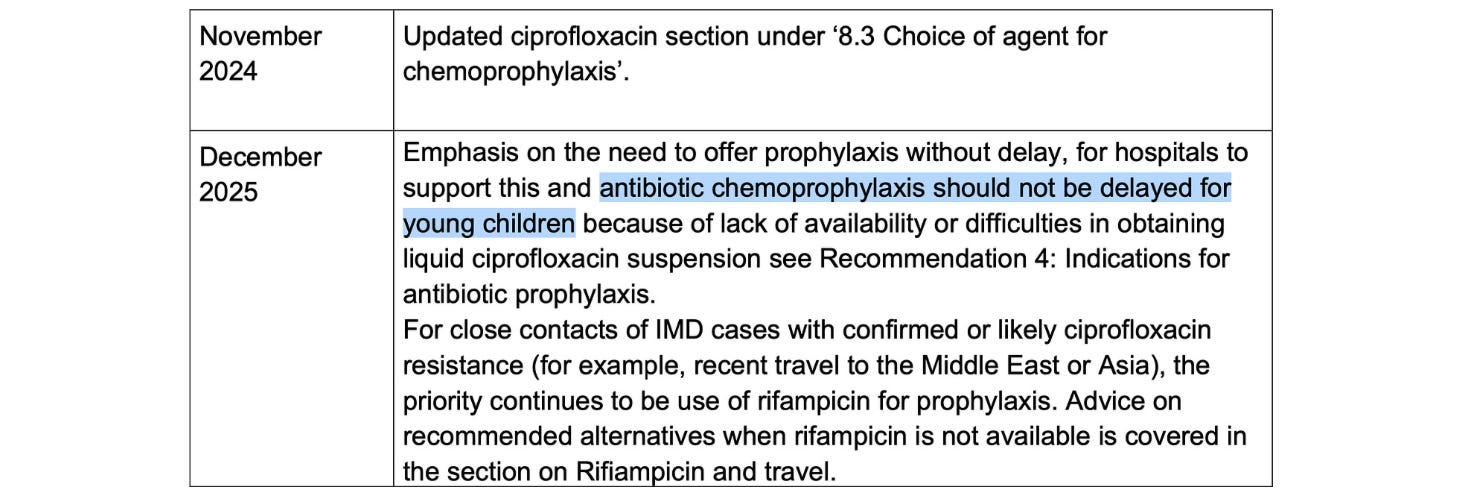
…which was updated last December to state:
…antibiotic chemoprophylaxis should not be delayed for young children…
But elsewhere, this UK government website has a stark warning from 2023 in relation to fluoroquinolone antibiotics such as ciprofloxacin (emphasis added):
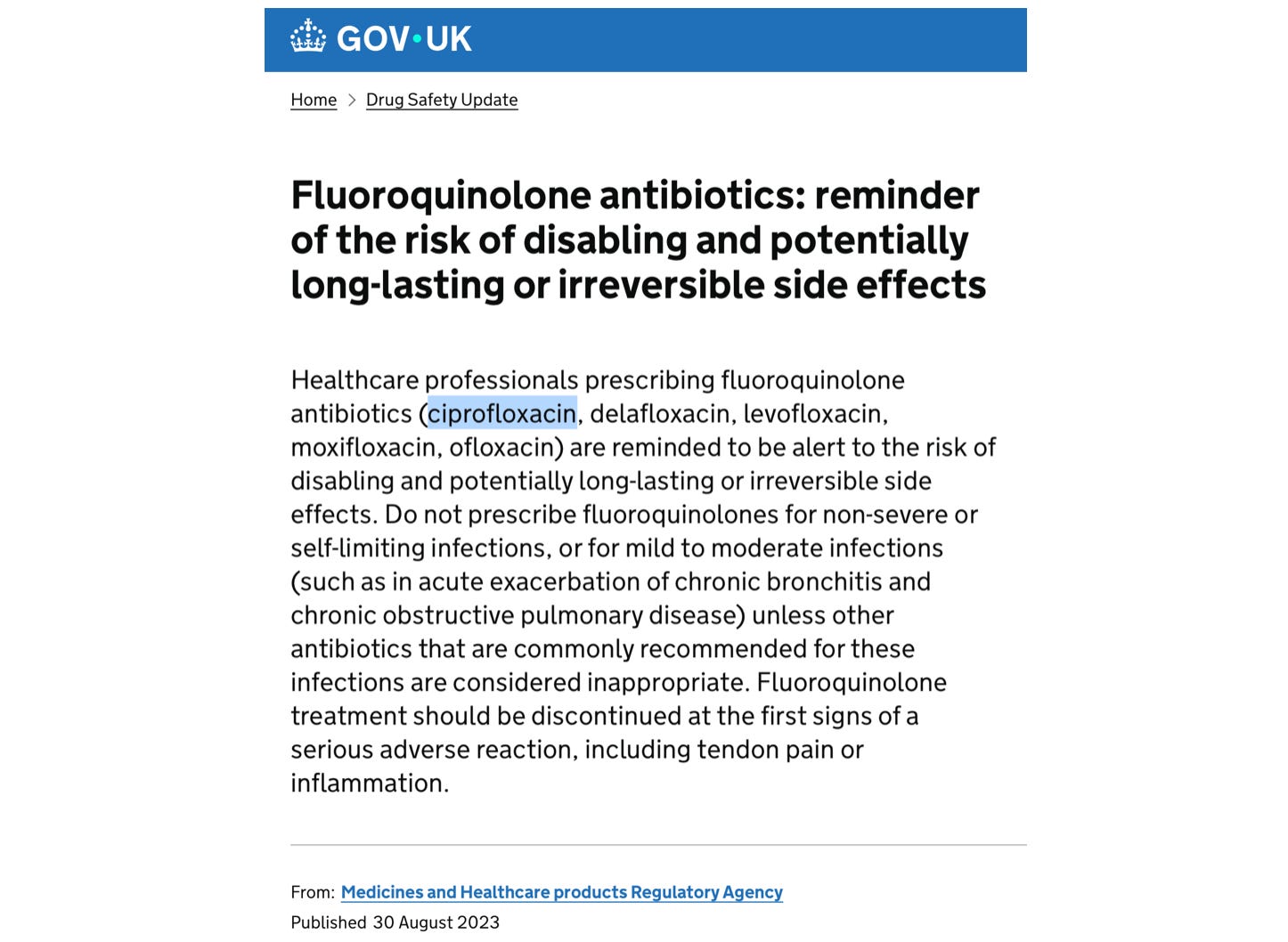
Healthcare professionals prescribing fluoroquinolone antibiotics (ciprofloxacin, delafloxacin, levofloxacin, moxifloxacin, ofloxacin) are reminded to be alert to the risk of disabling and potentially long-lasting or irreversible side effects. Do not prescribe fluoroquinolones for non-severe or self-limiting infections, or for mild to moderate infections (such as in acute exacerbation of chronic bronchitis and chronic obstructive pulmonary disease) unless other antibiotics that are commonly recommended for these infections are considered inappropriate. Fluoroquinolone treatment should be discontinued at the first signs of a serious adverse reaction, including tendon pain or inflammation.
Here is the reason:
Fluoroquinolone antibiotics have been reported to cause serious side effects involving tendons, muscles, joints, nerves, or mental health — in some patients, these side effects have caused long-lasting or permanent disability.
According to this 2008 British Medical Journal article, the FDA added a “black box” warning label to fluoroquinolone antibiotics such as ciprofloxacin:
In the context of this article in the The Guardian on 19th March which states that…
Health authorities have launched a major response: 30,000 people have been given antibiotics…
I asked Alter AI:
Tell me about the expected side-effects if 30,000 young people (late teens and early 20s) were given 500 mg ciprofloxacin as a single dose, including the rough numbers of those affected (100 words)
Here is the response:
If 30,000 young adults each took a single 500 mg ciprofloxacin dose, around 6,000–9,000 (20–30%) might get mild side effects — nausea (10%), diarrhea (5%), headache or dizziness (5–10%).
Roughly 300–600 (1–2%) could experience moderate effects — insomnia, anxiety, palpitations, or rash.
About 30–90 (0.1–0.3%) could develop serious issues — tendinitis, tendon rupture, peripheral neuropathy, or seizures.
5–10 people might suffer long-lasting or disabling fluoroquinolone toxicity, involving connective tissue and neurological damage.
Although most recover uneventfully, ciprofloxacin can unpredictably trigger persistent adverse reactions, especially in those with genetic mitochondrial fragility, prior antibiotic use, or concurrent physical stressors like intense exercise.
To be fair, the UK government does…
…advise patients to stop treatment at the first signs of a serious adverse reaction, such as tendinitis or tendon rupture, muscle pain, muscle weakness, joint pain, joint swelling, peripheral neuropathy, and central nervous system effects
…which is an improvement on the advice given to many of those who suffered an injury as a result of their first covid injection.
But it is worth noting here that some of the side-effects of ciprofloxacin (muscle pain, joint pain, peripheral neuropathy, and central nervous system effects) are not so very different from the early symptoms of meningitis (headache, feeling unwell, limb pain).
And that, according to the Cleveland Clinic, ciprofloxacin (emphasis added)…
…may cause serious skin reactions. They can happen weeks to months after starting the medication. Contact your care team right away if you notice fevers or flu-like symptoms with a rash. The rash may be red or purple and then turn into blisters or peeling of the skin. You may also notice a red rash with swelling of the face, lips, or lymph nodes in your neck or under your arms.
As to the 30,000 people who were given ciprofloxacin, I wonder how much of the above they were told.
Preventing transmission
According to this UK government website (emphasis added):
Around 10% of the population carries the meningococcus in the back of their throat or nose without causing any illness. It is transmitted from person to person by inhaling respiratory secretions from the mouth and throat or by direct contact (kissing). Close and prolonged contact is usually needed for transmission.
But that hasn’t stopped the mainstream media publishing articles like this:

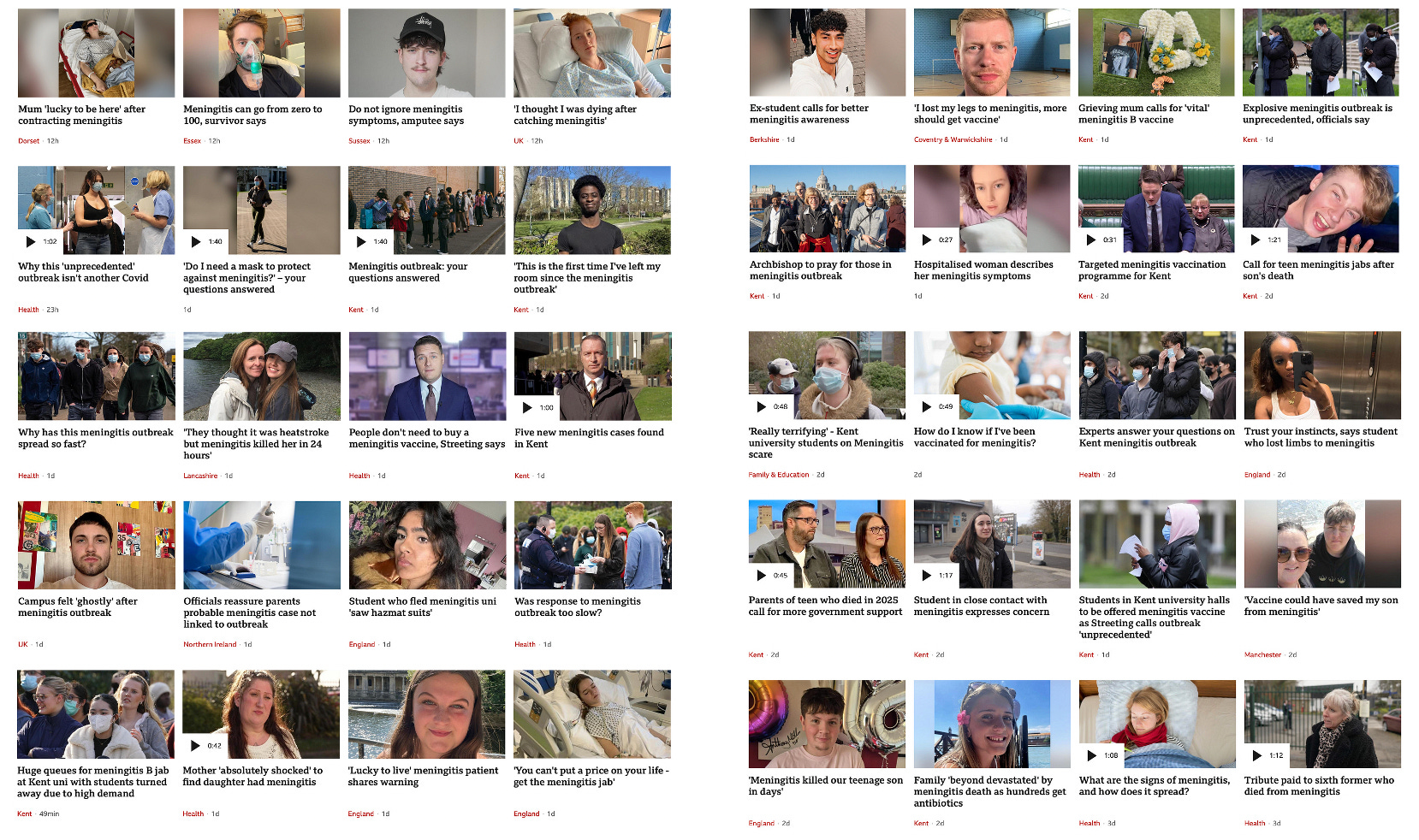
Or these (from the BBC News website search linked earlier):
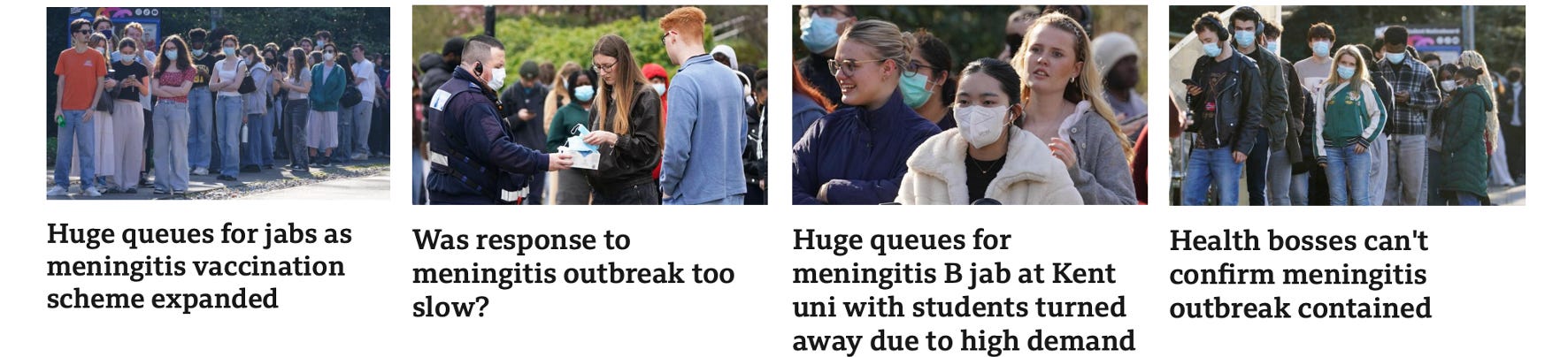
As far as I can tell, disposable face masks do more harm than good. And they are certainly disastrous for the environment. But there is a lot of money to be made from manufacturing, importing and selling them.
Moreover, and as behavioural psychologists know all too well, they are very effective at spreading fear. They also provide a visible sign (for better or worse) of who the non-compliant are.
I am reminded of this short covid era clip (transcript below) from Susan Michie, Professor of Health Psychology and long-standing member of the Communist Party of Britain:
Vaccines are a really important part of the pandemic control, but it’s only one part. The test, trace and isolate system [and] border controls are really essential. And the third thing is people’s behaviour, that is the behaviour of social distancing, of when you’re indoors making sure there’s good ventilation, or, if there’s not, wearing face masks… and hand and surface hygiene. We’ll need to keep these going in the long term. And that will be good not only for covid but also to reduce other…
And when asked by the interviewer, “When you say long term, what do you mean by that? How long…?” her reply was:
I think forever… to some extent…
I wonder to what extent behavioural psychologists have been involved in discussions around the reported meningitis outbreak.
The wearing of masks reminds me of another disastrous covid era intervention: lockdowns. There does seem to be, thankfully, a growing consensus that it was wrong during the covid era to enforce draconian restrictions on the freedom of the young in the name of protect the elderly.
But in April 2022 then Prime Minister Boris Johnson refused to rule out a future lockdown if a “more deadly covid variant” emerged:

And he particularly mentioned children in that context (emphasis added):
I’ve got to be absolutely frank with you, there could be… a variant that affects children, that we really need to contain… I’m not going to take any options off the table…
Exercise Pegasus
I am reminded of the UK government’s Exercise Pegasus from last autumn…

…which I featured in this post...

…in the context of the pre-Christmas hysteria over “Superflu”.
In November The Telegraph reported that Exercise Pegasus “imagined a virus deadly to children”…

…in which:
Schools across the UK were locked down…
And, coincidentally, we now have a meningitis outbreak in Kent several months on from Exercise Pegasus. I am reminded of how covid emerged several months after Event 201.
Vaccination
Another prominent feature of Exercise Pegasus was vaccination. And it is perhaps no surprise to see that around a quarter of the fifty or so BBC articles mentioned earlier make reference to meningitis vaccination in their title. Moreover, in the 24 hours since I took those snapshots of the BBC website, these additional articles have also appeared:

According to p45 of this UK Health Security Agency (UKHSA) guidance:

Two vaccines are licensed against MenB; 4CMenB (Bexsero®) and rLP2086 (Trumenba®). The vaccination dosing and schedule for 4CMenB (Bexsero®), as well as the licensed age indication, is in general more suitable for cluster/outbreak control than rLP2086 (Trumenba®).
A summary of the trials conducted on Bexsero (and Trumenba) can be found here:

Like most childhood vaccines, the clinical trials were short, and neither used a genuine placebo. In the case of Bexsero, the GSK vaccine considered generally more suitable for cluster/outbreak control:

A single dose of MENVEO [another meningitis vaccine] was administered as a control…
Here is the dose recommendation for Bexsero:

Adolescents (from 11 years of age) and adults should receive two injections of the vaccine.
And
The interval between each injection should be at least 1 month.
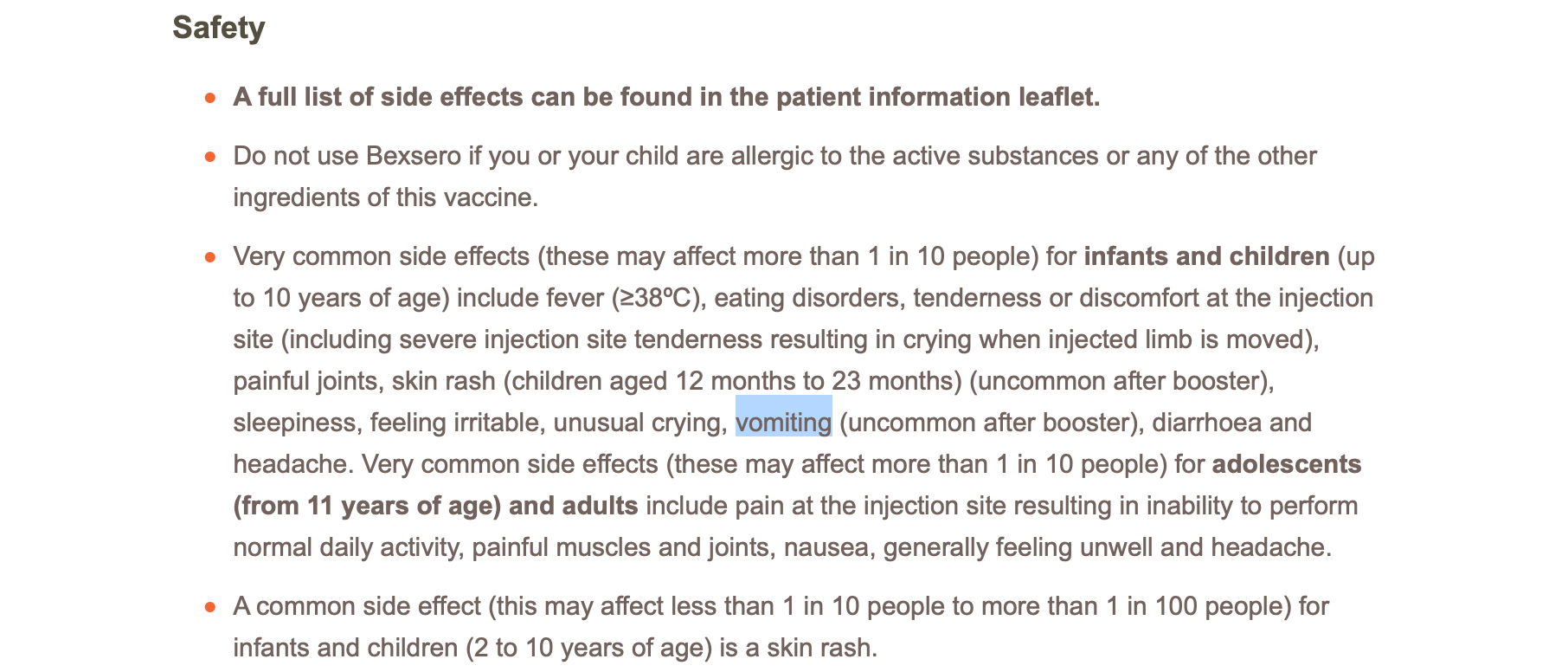
“Very common” side-effects (affecting more than 10% of those injected) include…
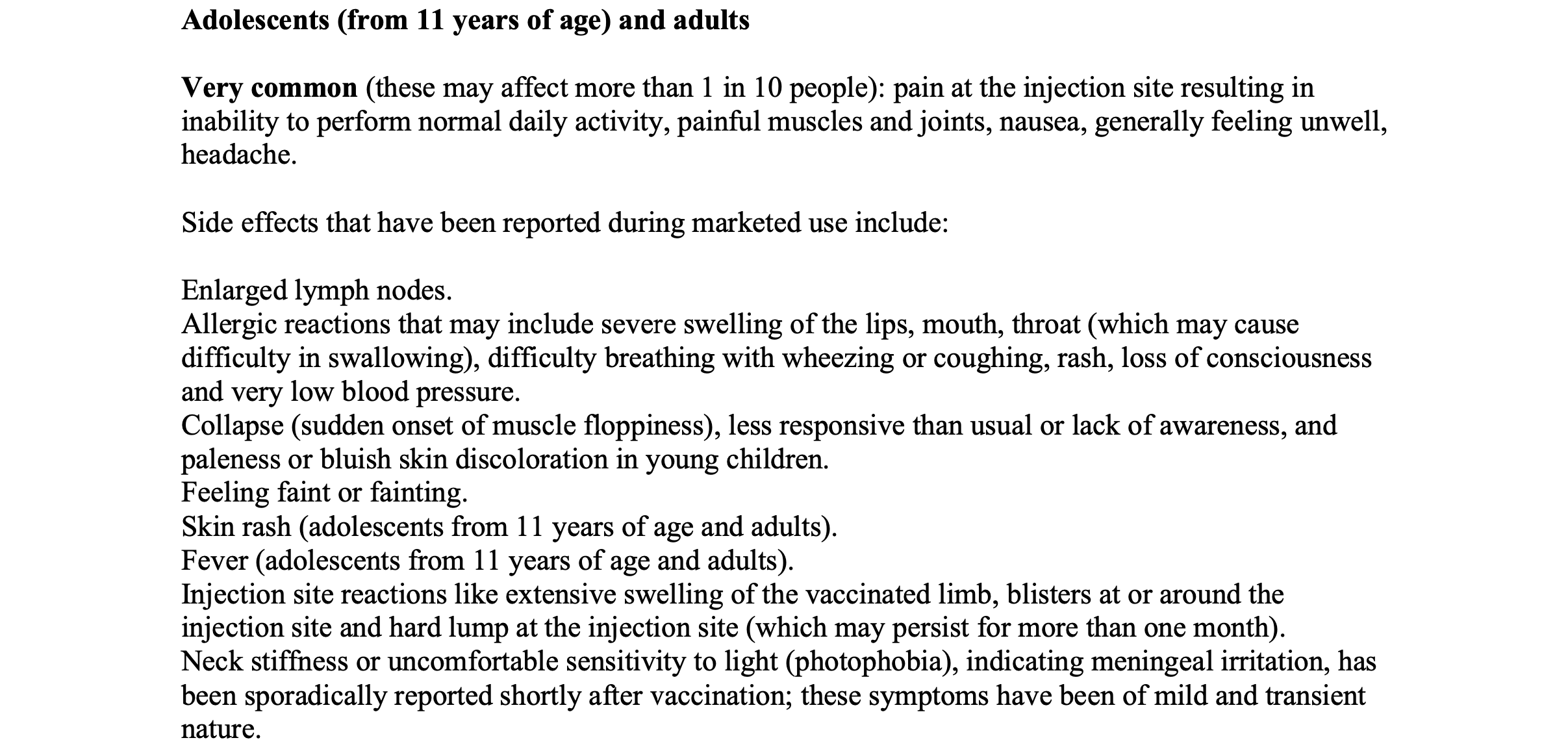
…painful muscles and joints, nausea, generally feeling unwell, headache.
Other side effects that have been reported during marketed use include:
Enlarged lymph nodes.
Allergic reactions that may include severe swelling of the lips, mouth, throat (which may cause difficulty in swallowing), difficulty breathing with wheezing or coughing, rash, loss of consciousness and very low blood pressure.
Collapse (sudden onset of muscle floppiness), less responsive than usual or lack of awareness, and paleness or bluish skin discoloration in young children.
Feeling faint or fainting.
Skin rash (adolescents from 11 years of age and adults).
Fever (adolescents from 11 years of age and adults).
Injection site reactions like extensive swelling of the vaccinated limb, blisters at or around the injection site and hard lump at the injection site (which may persist for more than one month).
Neck stiffness or uncomfortable sensitivity to light (photophobia), indicating meningeal irritation, has been sporadically reported shortly after vaccination; these symptoms have been of mild and transient nature.
Fever, joint and muscle pain, rash, fever, headache, neck stiffness…
Compare and contrast those side-effects with the list of meningitis symptoms at meningitis.org:
NB GSK’s Bexsero information also lists vomiting among the very common side-effects for the vaccine:
Moreover, here are a couple of snapshots of the Bexsero prescribing information from the US Food and Drug Administration (FDA) website:
On page 2…

BEXSERO may not protect all vaccine recipients…
And on page 9…
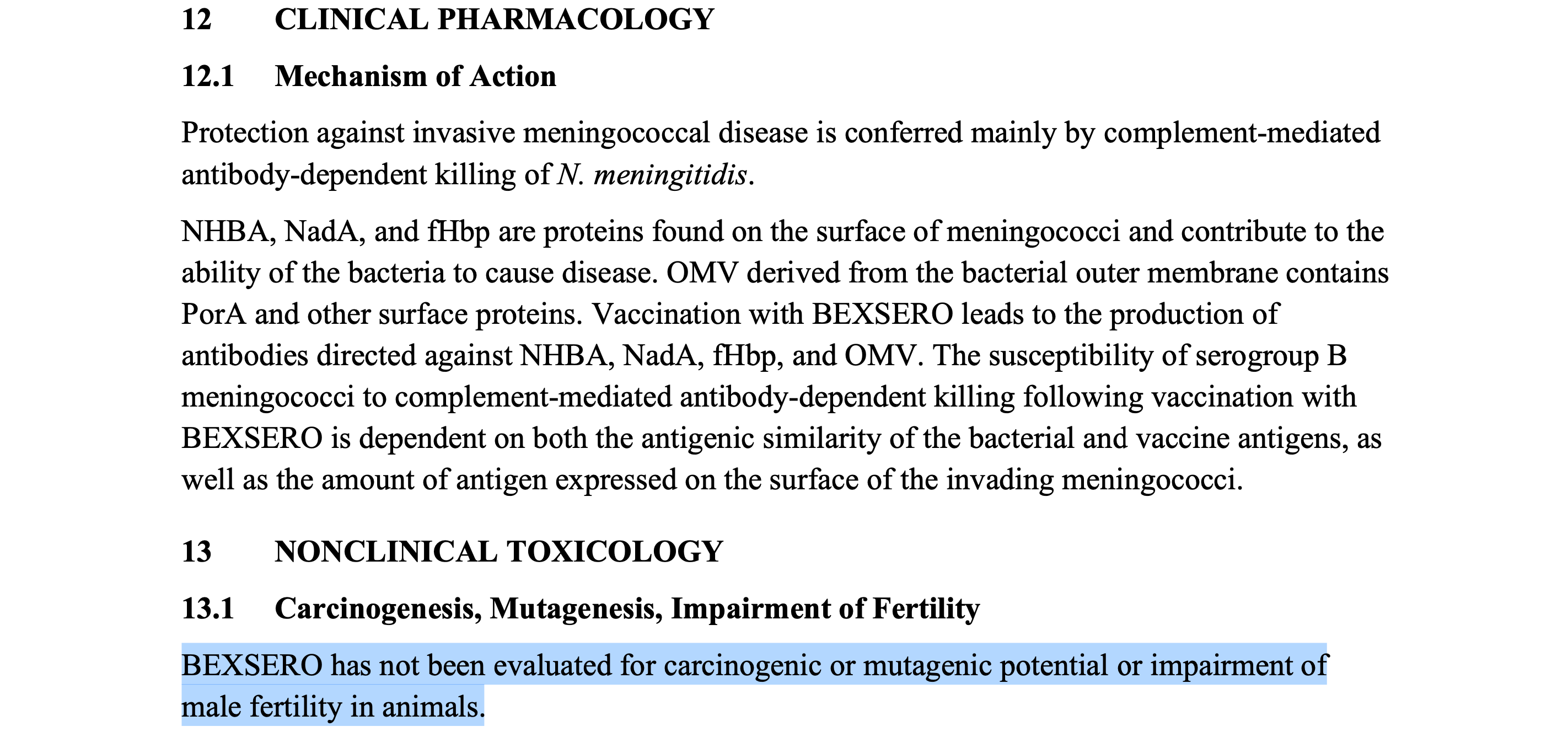
…under the heading of Carcinogenesis, Mutagenesis, Impairment of Fertility:
BEXSERO has not been evaluated for carcinogenic or mutagenic potential or impairment of male fertility in animals.
In other words, tests have not been done to investigate whether the vaccine might cause cancer, alter genetic information, or have a detrimental effect on male fertility.
I wonder how many of the people who have received one or more Bexsero injections are aware of that.
But none of the above is putting off the authorities in their zeal for vaccination (emphasis added):

Given the severity of the outbreak, and as an additional precautionary measure, a targeted vaccination programme will begin, starting with students that are residents of the Canterbury Campus Halls of Residence at the University of Kent who will be contacted directly.
“An additional precautionary measure”. To go with the antibiotic chemoprophylaxis. For your safety.
The aforementioned article in The Guardian states that…
…up to 5,000 University of Kent students will receive a meningitis B vaccine
On the plus side, at least I don’t recall seeing anyone describe these injections as “safe and effective”.
Finally, I was intrigued to see this webpage on the UK government’s Find a Tender website:
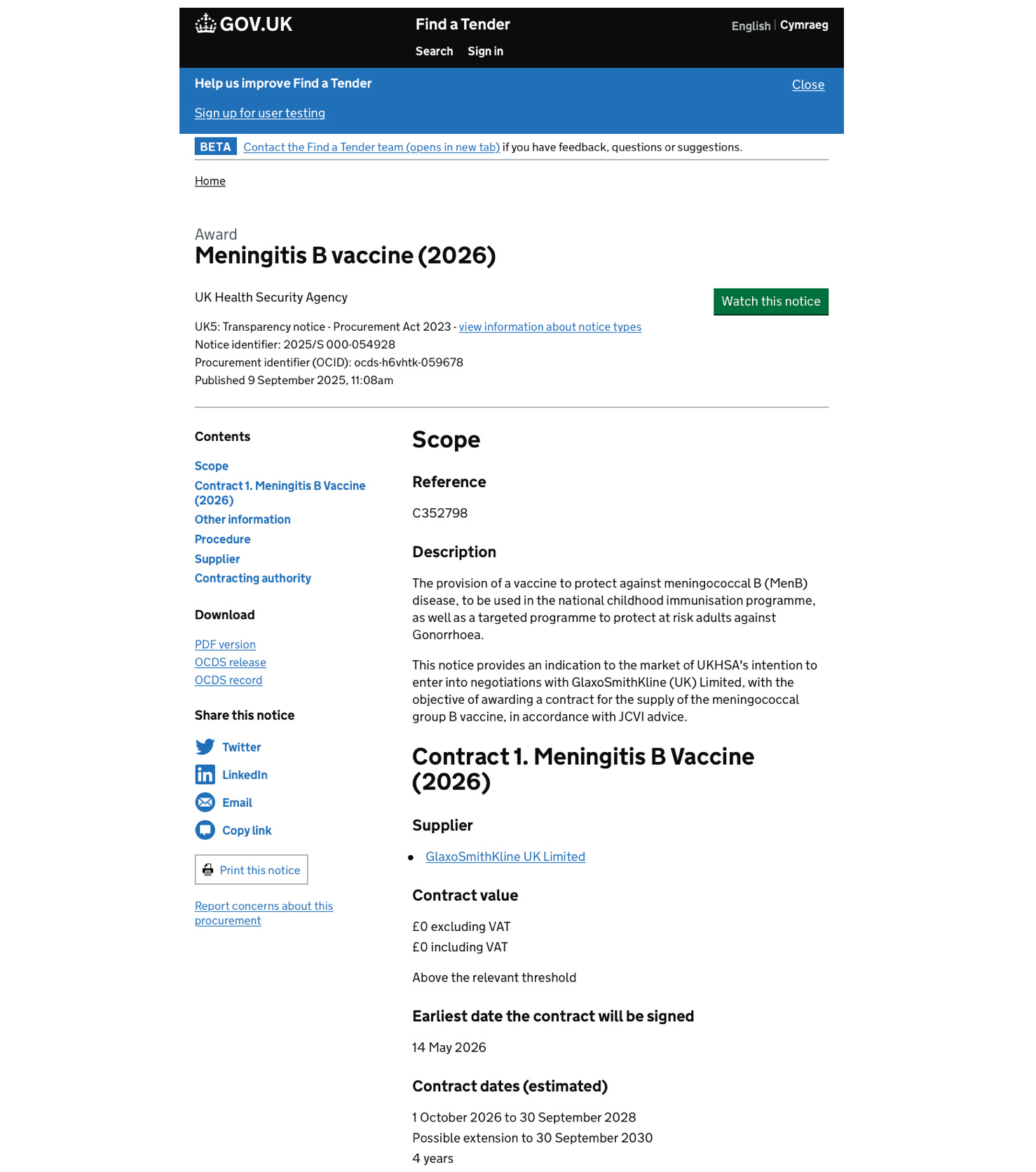
Contract 1. Meningitis B Vaccine (2026)
Value apparently to be determined.
Supplier: GlaxoSmithKline UK Limited [GSK]
Contract dates (estimated): 1 October 2026 to 30 September 2028… possible extension to 30 September 2030
Make of that — and the rest of the above — what you will.
Related:


![A wolf in sheep's clothing [2025 re-issue]](https://substackcdn.com/image/fetch/$s_!S3sp!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F7c57acd2-6e50-4a94-ba6a-5450590f16db_908x786.png)

![Reflections on fear [2025 re-issue]](https://substackcdn.com/image/fetch/$s_!sp7x!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F27f6fa75-1343-49cc-836e-5d9dcef41ad7_882x856.png)





Dear Church Leaders (and everyone else) homepage
Some posts, including a version of this one, can also be found on Unexpected Turns
Revealing Faith: Seeing and believing the revelation of God
The Big Reveal: Christianity carefully considered as the solution to a problem
Which I first cited in here in The first person to speak seems right until someone comes and asks the right questions