Part IV: inconvenient truths about myocarditis; higher incidence of myocarditis after the covid vaccine (not covid); a 20-year-old with covid vaccine-induced myocarditis; MHRA withholding data...
…in which the purpose was to convey a flavour of what has been going on during Module 4 of the UK Covid-19 Inquiry…
Below are four short videos about heart damage, along with transcripts.
NB myocarditis is inflammation of the heart muscle.
IV-1. Inconvenient truths about myocarditis [link]
Contributor: Dr Ros Jones, retired NHS Consultant Paediatrician
[Emphasis added]
[Dr Jones] I got together a group… some of you are here, but we’ve now got over 200 senior, experienced health professionals and academics. And we were writing repeatedly to the regulators, the politicians — you name it, we’ve written to them.
We were most concerned about myocarditis with 16-25s at highest risk It’s on the patient information leaflet, but we keep being told it’s “very rare” and it recovers quickly.
For context, terms like “very rare” do actually have formal definitions:
Very common: Affects more than 1 in 10 people (≥ 10%)
Common (frequent): Affects 1 in 10 to 1 in 100 people (1–10%)
Uncommon (infrequent): Affects 1 in 100 to 1 in 1,000 people (0.1–1%)
Rare: Affects 1 in 1,000 to 1 in 10,000 people (0.01–0.1%)
Very rare: Affects fewer than 1 in 10,000 people (< 0.01%)
The video then features a brief exchange from the UK covid inquiry:
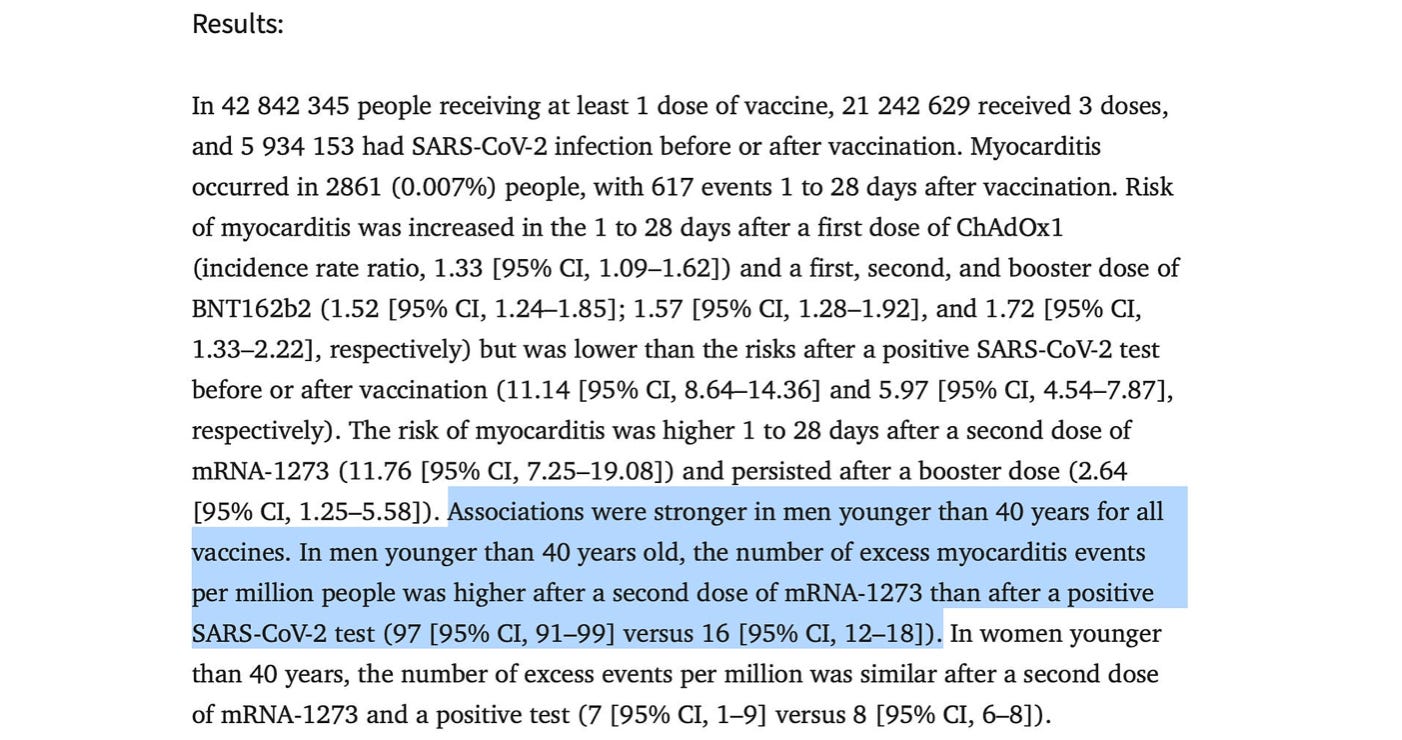
[Hugo Keith, lead lawyer] Does the data suggest in fact that whilst there is a risk of myocarditis after vaccination, the risk was much lower compared to that seen following covid infection in the unvaccinated. And I should say that’s the conclusion from one particular study to which you refer. Was that outcome, that proposition consistent with the generality of the material you looked at?
[Dr Alhambra, witness] That is correct, and I would say this study in particular by Patone et al is probably one of the best-quality studies on this topic.
Dr Jones asks:
Did Dr Alhambra actually read the study he quoted? The results section showed that for men under 40, the risk of myocarditis following their second vaccine dose was six times higher than after infection.
How rare an adverse event is also depends on how hard you look for it. Israel’s passive reporting system had around 1 in 6,000 teenage boys affected, but Thailand did what the MHRA should have demanded of Pfizer — a proper prospective study. Two big secondary schools gave pupils diary cards and blood tests and ECGs before and one week after their second dose. They found a very worrying 1 in 29 of the boys with subclinical or clinical myo- or pericarditis.1So that, for Mr Keith’s information, is common.
As for “mild… gets better quickly”, teenagers admitted to US hospitals in Summer 2021 with chest pain and palpitations after their vaccines did indeed seem to settle within days. But they were all given a cardiac MRI scan, and 89% had changes suggestive of scarring to the heart muscle. And in 60% of them, these changes were still present six months later. This type of scarring has been associated with reduced five-year survival.
We wrote to the regulators… we wrote to three consecutive prime ministers. We got no sensible answers; and so… we’ve been trying to share all our information with parents, and that’s probably the most useful thing we’ve done.
During 2020, the “year of the pandemic”, Google searches for myocarditis were at close to normal levels.
It was not until around May 2021 that interest began to rise significantly:
IV-2. Higher incidence of myocarditis after the covid vaccine (not covid) [link]
In Guernsey, every five years I would get perhaps one serious case of myocarditis… When covid came along, we were told that myocarditis was a serious complication in 5% of people. And with a population of 63,000 we had quite a tough lockdown in Guernsey, so we didn’t have a huge wave in 2020. However, there was still a significant burden of covid. I had sick people out of intensive care, being on ventilators for three months, and, before the vaccines were released, I believe around 2000 people that were infected.
So if you say 5%, which is what the UK government says is the risk of myocarditis post-covid, then we’re dealing with between 50 and 100 people that I should have become aware of having myocarditis from covid. But I don’t recall seeing one patient. And even the sickest patient coming out of intensive care, who had been kept alive on adrenaline for three months, he had zero evidence of myocarditis… cardiac ultrasound was normal. So I honestly cannot tell you that covid causes myocarditis. If it did, I’d be concerned, wouldn’t I? Because you would naturally assume that in my role as a cardiologist I would be wanting to help prevent people getting injured from the covid virus causing myocarditis.
It was [not] until the vaccine came out that I saw [myocarditis] flare up. And it was impossible for me not to see it because… patients were presenting with problems. And so I had 25 cases in 2021. There were a lot of patients with pericarditis and chest pain. I have a list of 20, but the list is greater than that because it’s impossible running my day job… trying to keep track of all numbers. In 2022 we’ve had another 22 cases and in 2023 we’ve had 11. But there are 19 cases I’m waiting on further assessments because I get cardiac MRI on all these patients as part of their final assessment.
I think there’s been 5 deaths and about two or three of those deaths have not been clearly documented. I remember one patient of mine… he had nine cardiac arrests in a 24-hour period. So despite everything that we were doing for him, he was constantly going into cardiac arrest. And at the time he ended up being treated with a defibrillator. He never got formally assessed as to whether he had myocarditis, but despite everything that we did for him he ended up just dying a few months later.
The population of the UK is around 1000x the population of Guernsey.
IV-3. A 20-year-old with covid vaccine-induced myocarditis [link]
[Dr Patterson] This is a young man who I saw in 2021, and he developed what was indistinguishable from an acute myocardial infarction.2 The only difference is [that] in a 20-year-old there are very, very rare occurrences when a 20-year-old will have a myocardial infarction; but in this particular case, he developed a very early post-vaccine myocarditis which was extremely severe:
[Bilal Asif] My name is Bilal Asif. I’m 20 years old. I had the covid jab booked in for the morning, so I went into work for an hour. 10am… I went for the vaccination. I cycled to Beau Sejour, sat down, waited. I had the vaccination, but during that time at work, I developed a rash that night… all over my arms… on my lower legs, the side of my ribs. I went to sleep as normal.
The next day I had chest pains. I didn’t think much of it at first. I thought it was just a chest problem, coughing, but it slowly, gradually worsened over the day. And then I went to bed with the chest pains as well, again, and I tried to sleep it off. I thought maybe the next day I’d be fine. But at that point it was so severe it woke me up. It was unbearable… so I phoned the ambulance.
As soon as I got to the hospital I was pretty certain that it was the vaccine. I’d never gone through anything like that before. After I’d been admitted… the pain had gone away. But… it was the day after… I’d arrived… the chest pain had returned but this time it was quite severe. The pain was so bad I was shaking. It definitely felt like it was a heart attack and it felt like my heart was coming out of my chest.
[Dr Patterson] In any other age group above 35 years of age, the knee-jerk reaction will be this patient’s having an acute myocardial infarction. And that will be managed as such, which in most centres would be an ambulance directly to what’s called the coronary catheter lab, where you would be examined to make sure there’s no thrombosis (clotting) within your coronary arteries.
And during that period in 2021, and even 2022, there is still the post-lockdown… covid management. There is a lot of pressure on the NHS having come through huge backlog from lockdown. And so patients were very much in and out: “Do you need a treatment for a coronary stent, or not?” And I believe that a lot of patients with myocarditis would have been discharged and not thoroughly assessed because of the pressures on the NHS and because also at that stage everybody was told that it’s covid causing the myocarditis… like a post-war situation where you are shell-shocked, where people just stop thinking correctly.
This chart is from p20 of this UK government covid vaccine surveillance report at the end of 2021:
The font is small, but the data shows that many people aged 18-40 received their first covid injection during May-June. And their second in August-September (see p21).
Here is a chart showing the level of interest in myocarditis as a Google search term during 2021:
Here is the British Heart Foundation covid vaccine webpage at the time of writing (March 2025):
In the BHF’s Annual Report and Accounts 2024, I couldn’t find details of which particular organisations or individuals the charity receives money from, but there is this comment (on p110) in relation to fundraising:
I wonder what it would take for an organisation like the BHF to advise against having covid injections.
IV-4. MHRA withholding data about increased heart conditions in the covid-vaccinated [link]
Contributor: Nick Hunt, retired Senior Civil Servant from the Ministry of Defence who was responsible for the safety and effectiveness of a wide range of explosives
[Emphasis added]
And here’s another key safety issue which the inquiry completely ignored.
All three companies — Pfizer, Moderna and AstraZeneca — were all required to do post-authorisation safety studies. And this involves analysing NHS data on millions of people, segmented by lots of factors like age, gender, socioeconomic background… but importantly, covid vaccination status.
And this is to explore if the covid vaccines have increased the incidence of a specified long list of adverse events, health conditions. Now we included in our written evidence to the inquiry that Pfizer’s Interim Report 5 was completed in March of last year but that MHRA was withholding publication [and] that we had obtained a summary of that report from another source. And, moreover, that that summary reports a significantly higher incidence of heart conditions among the covid vaccinated. The inquiry completely ignored that evidence.
What it should or could have asked is: “Why is MHRA still withholding publication?” And here I have to note that June Raine in her evidence said, under oath, that MHRA was not sitting on any such post-authorisation reports.
Why did the inquiry expert witnesses — or at least one of them — Professor Alhambra… why does he say that the increase in heart conditions is not caused by the vaccines when Pfizer in that report is obviously saying it is causing that increase in heart conditions?
Another good question would be: “Has MHRA required the covid vaccine manufacturers, or indeed any other research body, to extend the analysis of that NHS data to other conditions?” And let’s just start with cancer for example, rates of which are known to have increased significantly… into which I think [Prof] Angus [Dalgleish] is going to speak…
A clip of Prof Angus Dalgleish speaking at the People’s Vaccine Inquiry is featured here.
For analysis of UK data into other conditions, see e.g. this work from Phinance Technologies — two PhD physicists working with former hedge fund manager Ed Dowd to examine the yearly numbers of UK PIP clearances:
NB PIP = Personal Independence Payment — “benefits and financial support if you’re disabled or have a health condition”:
On this part of the Phinance Technologies website, you can click on the list of areas in the bottom left corner and generate data for the yearly numbers:
The rises for e.g. “Haematological” (blood-related, pictured above), “Psychological”, “Neurological” and “Musculoskeletal” are substantially larger than for those for “Oncology”.
This table further down the same page is also interactive, and provides a summary of the numbers from 2016-2022:
If you haven’t seen this short post featuring Ed Dowd, I recommend it:



![[I] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F8388da85-e410-4fb8-8058-3b7d2f0bde3a_748x730.png)
![[II] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F1796b701-1eeb-4906-83ad-572a867613fc_858x864.png)
![[III] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F9e38efc4-8d0d-4188-b4b4-afb7b0547e8d_872x838.png)















![[V] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F5fbe5bd2-1d3b-4566-996b-c459a24c4762_780x796.png)





