"Less is more"
Remarkable results in cancer patients taking a low-dose, low-cost and low-risk drug that is on the WHO Model List of Essential Medicines
Dear Church Leaders (and everyone else)
In the podcast featured in this post…

…the discussion ends with UK oncologist Prof Angus Dalgleish stating:
If I [were] the Chief Medical Officer… the first thing I would do with everybody… [would be] to get them to have a test [for covid spike protein] and then have trials to see how can we get [the level of spike protein] down to zero.
There’s no end of [drug] candidates… [that aspect] is very easy… My own [preference] is low-dose naltrexone [which is used in the management of alcohol and opioid use disorders] which I’ve been working on for 20 years… and we find that it’s a very good way of reducing inflammation through the IL-6 pathway… [We’ve] been doing it in cancer and… we were the first to show [that naltrexone] suppresses the IL-6 inflammatory pathway. [And] what was the inflammatory pathway of covid? IL-6. [And] what is the determinant of “long covid”… which is [actually] “post-vaccine covid”…? That’s the only “long covid” you’re going to see now…
And further to this follow-up article focusing on the part of the podcast discussing the use of ivermectin, fenbendazole and mebendazole for cancer treatment…

…I thought it worth sharing this recent video where Prof Dalgleish talks more about naltrexone.
The interviewer is former clinical nurse Dr John Campbell.1 A transcript of the most relevant parts can be found below, along with occasional additional links and notes.
[Campbell] Tell us a bit about low dose naltrexone…
[Dalgleish] Low-dose naltrexone is a wonderful story in itself and it would make a very good film actually…
It was discovered by total serendipity by… a Dr Bihari who ran the drug addiction program in New York… He noticed that when they tried naltrexone… to wean you off morphine and heroin addiction… in about half the patients it actually… did work… they had benefit.
Here is Dr Bernard Bihari discussing the development of low-dose naltrexone:
[Dalgleish] And because of the nature of the drugs, they rolled off the dose… you don’t stop [straight away]… you just keep [reducing] it… And [Bihari] was bright enough not to dismiss people saying, “Can I stay on the low dose?” He actually said, “Why do you want to stay on the low dose?”
And… people said, “Well…I have MS [multiple sclerosis] and it’s much better on the low dose…” or “I have Crohn’s disease and it’s much better on the low dose…” or “I’ve got arthritis and it’s much better…” And he actually listened… unlike any of the doctors I know these days… they just dismiss [such illness] as… inflammatory…
So it was all [documented]… [Bihari] collaborated with Dr Zagon in Philadelphia, and they showed that the low doses altered opiate receptors. They’re not high enough dose to block them. They alter them… modulate them… and this results in a… change in neuropeptides affecting the endocrine system and the immune system…
Here is Dr Ian Zagon’s Researcher Profile from the PennState Cancer Institute website:

He is also the editor of the journal Multiple Sclerosis:
[Dalgleish] Well, I got involved because I found an obstinate patient who wouldn’t tell me why they were doing so well when we’d run out of options… and [who] finally told me she was getting low-dose naltrexone from Dr Bihari. And I went over [to the US]… [to discover] whether this was smoke and mirrors, fraud or… there was something in it that we didn’t understand. I came to the conclusion it was the latter. I think you have to meet these sort of people to work out how likely it is that you’re dealing with somebody who recognises these things and understands...
And so I started giving [low-dose naltrexone] to my oncology patients [in the UK] who’d run out of options but weren’t ill enough to go to palliative care… which is actually quite a [lot of them]… And we then started noting that we were getting rather overwhelmed… having to do repeat three-monthly prescriptions. And… I thought this person was going to be dead in six months and [yet] I’m still doing prescriptions in the second year…
And then I decided to haul some of these people back and re-scan them. And I found that in some of the cases… multiple liver [secondary cancers] hadn’t progressed at all since going on low dose nalprexone… We then started to see some absolute responses. They’re rare… the stabilisation seems to be very, very common, but [absolute] responses a bit rarer… And I came to the conclusion [that] no amount of fiddling with opiate receptors and neuropeptides can do this. There’s something else going on. So that’s when I decided… [the drug] must be using another receptor… another pathway.
So I used my old HIV receptor knowledge and techniques, and I decided the best way to go fishing is to get a net… [And] I got every single immune receptor in the book assembled for a big fishing expedition… and [it turned out that] the low-dose naltrexone inhibited TLR9 and [TLR7 and TLR8 a bit]… this toll-like receptor [TLR] inflammatory pathway… a major inflammatory pathway which, when you stimulate it, produces IL-6…
When [the discovery of] IL-6 [interleukin 6] was published… I remember reading the paper… it was called… the cancer growth factor.
According to thefreedictionary.com, an interleukin is a substance extracted from white blood cells that stimulates their activity against infection and may be used to combat some forms of cancer.
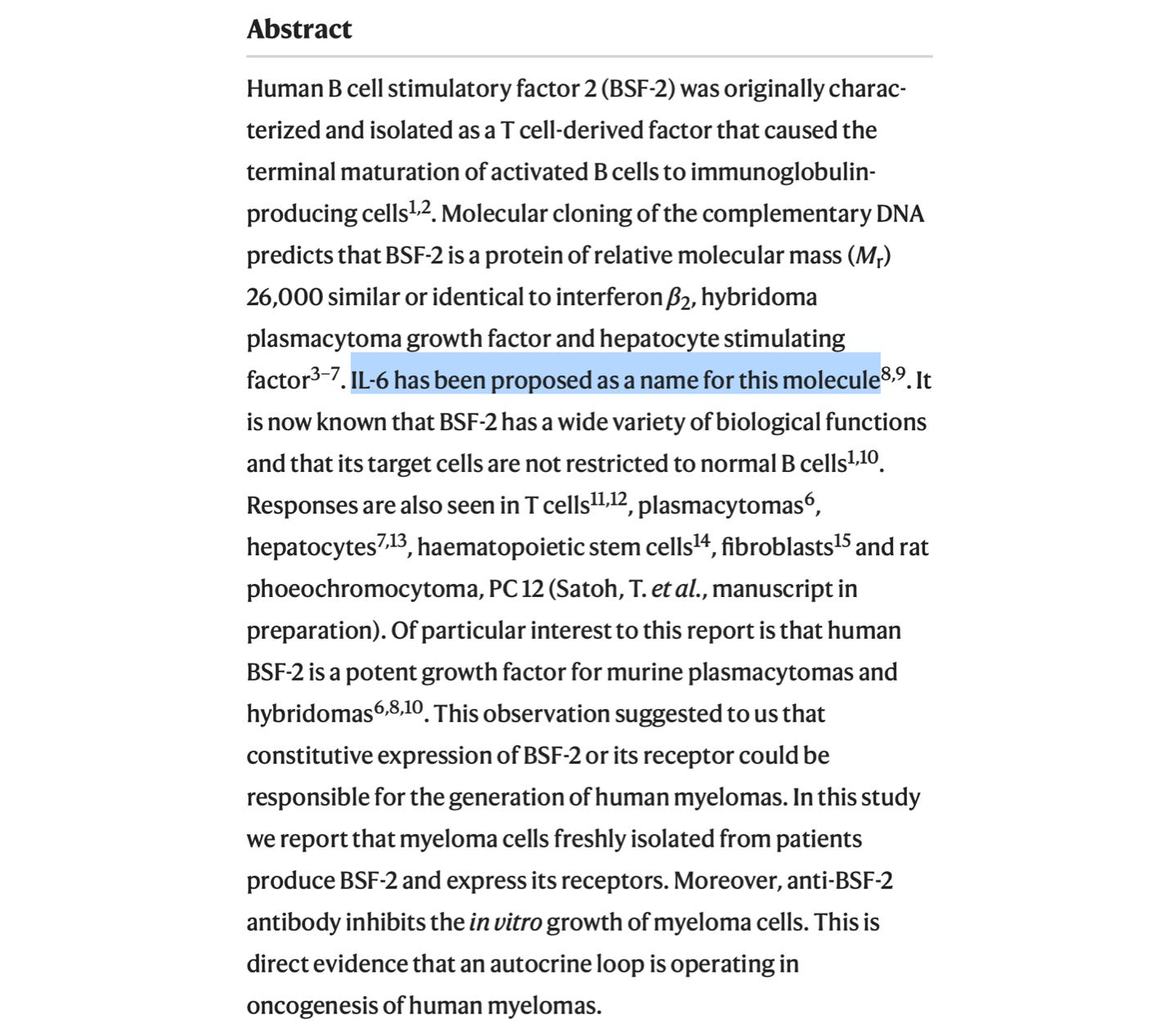
Here is a letter published in Nature in 1988 mentioning the naming of IL-6:

[Dalgleish] So I thought… we’ve got a drug [taken] orally once a day that switches off [a] cancer growth factor…
And to give you an idea how relevant it is… two companies make antibodies to IL-6… When you’re very [far] advanced with cancer, you can get these £100,000 drugs… And that’s another insight to what’s going on with Big Pharma… They’re not interested in something cheap… that will actually improve everything… The checkpoints [with antibodies] were costing about $100,000 a year. And they were wanting to give two years worth to everybody with melanoma just in case…
[Yet] it would cost [next to] nothing to put all those who needed it on low-dose naltrexone…
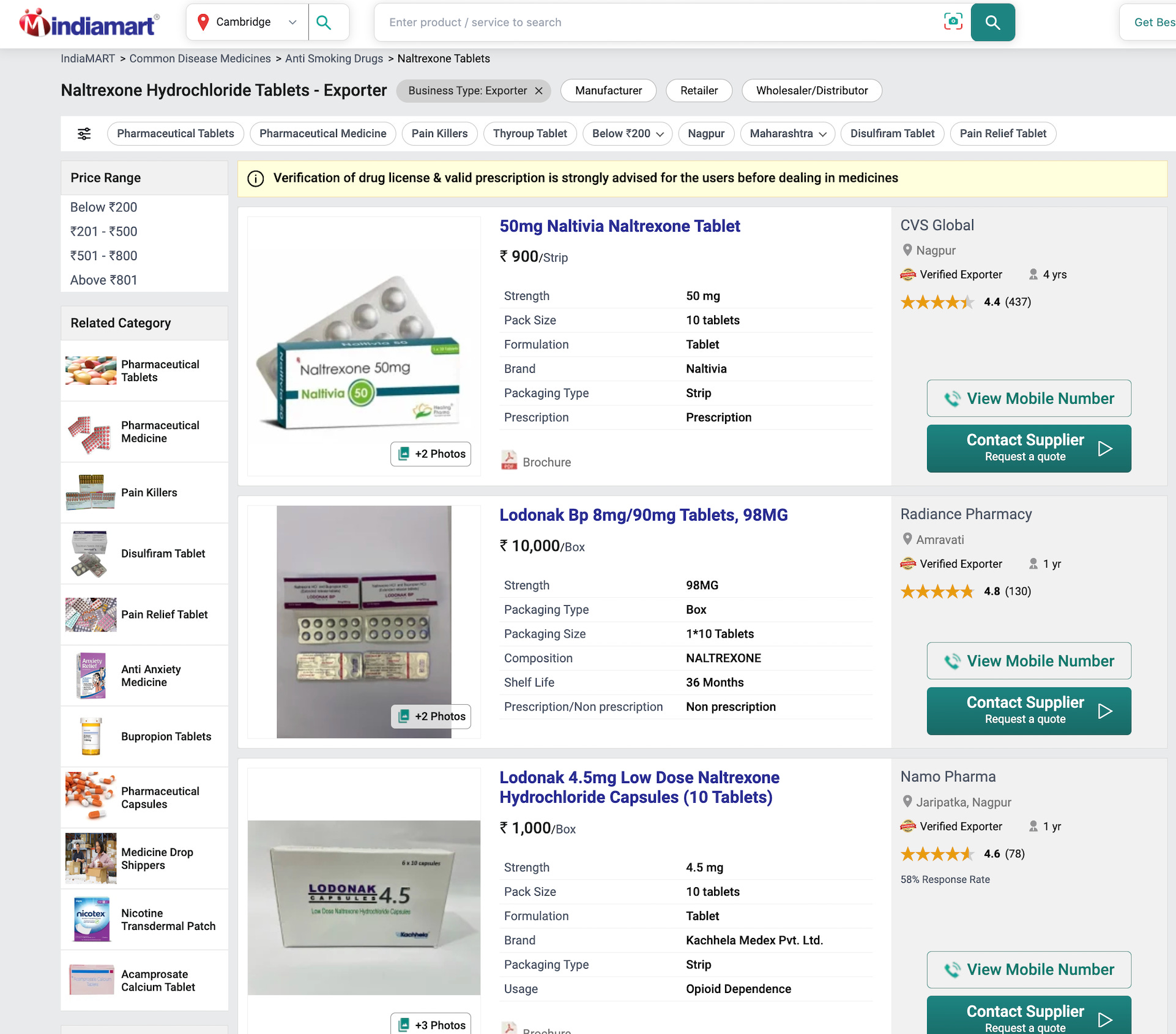
Indiamart offers 10 x 4.5 milligram tablets for 1,000 rupees (about £8):
1mgstore.com has 30 x 50 milligram naltrexone tablets for $96.
[Campbell] What sort of dose… would I need?
[Dalgleish] 4.5 milligrams absolute maximum… and a lot of people… find the benefit even better at 3 milligrams. So… if you’re 70 kg or below you have 3… If you’re over 70 [kg] you have 4.5… and bear in mind there’s individual variation. So that’s the range… but never go over 4.5.
Any side effects [with low doses come] very early on… it involves sleeping and dreams… which is why they suggest starting even lower… [going] to 4.5 over a couple of weeks. But I’ve never had anybody not be able to take [low-dose naltrexone] because of sleeping and dreams… it attenuates [and] settles down eventually.
[Campbell] For treating heroin addiction, what were we using? 25… 50 milligrams…? So this is [a very] small dose isn’t it?

[Dalgleish] Exactly…
[Campbell] It’s a bit like aspirin. After a coronary event we’ll give 300 milligrams of aspirin, but that works way better than 600 milligrams of aspirin. So it’s a matter of optimising the dose, and that’s often a lower dose…
[Dalgleish] Actually, what it woke me to… both low-dose naltrexone… and IMM [IMM-101, a recently-developed immunotherapeutic agent used in cancer treatment]… these are both drugs which if you looked at the starting dose… they fail… they won’t work. Usually in drug development when that happens you increase the dose, but in both these cases it is the reduction…
With… IMM-101… when they gave it intra-dermally, it didn’t work very well first of all. So they look at everything… how it’s made… what have you… And the big secret was… if you actually reduce the day the dose by 90% and just gave 10% of it... it worked perfectly… These are both drugs showing that less is more. They work far better in low doses than high doses.
Not unrelated:


Dear Church Leaders (and everyone else) homepage
Some posts, including a version of this one, can also be found on Unexpected Turns
Revealing Faith: Seeing and believing the revelation of God
The Big Reveal: Christianity carefully considered as the solution to a problem
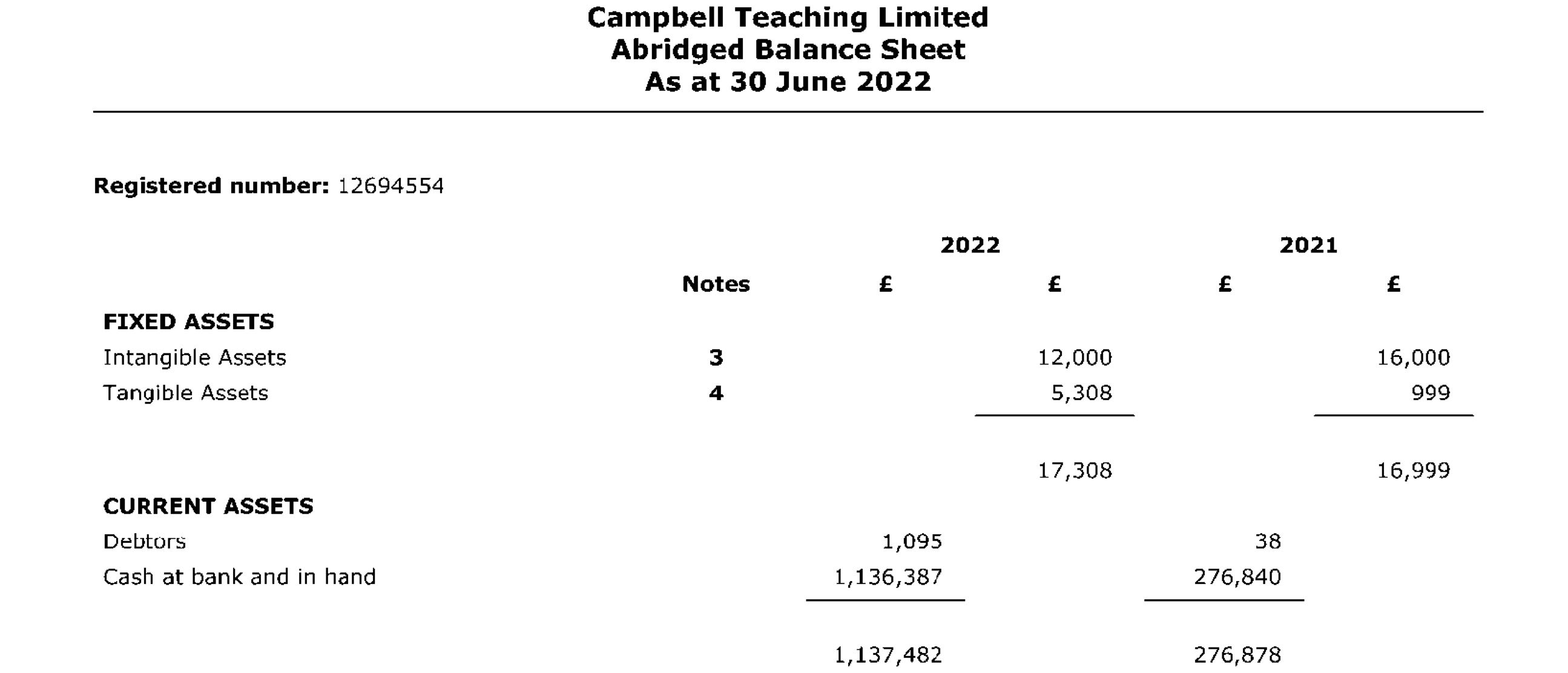
For the record I do share concerns about John Campbell such as those raised e.g. in this post by Jonathan Engler. Companies House has this abridged balance sheet for Campbell Teaching Limited in mid-2022 after Campbell had been promoting covid vaccines (h/t ThinkingCoalition):