


Recent revelations
Recently-released meeting minutes of the Vaccine Benefit Risk Expert Working Group; minutes re the covid vaccination of children (obtained by a Freedom of Information request)
Dear Church Leaders (and everyone else)
As it happens, since this recent article…

…light has been shed on some key government meetings held during 2020 and 2021.
Recently-released Meeting minutes of the Vaccine Benefit Risk Expert Working Group from the Covid-19 Pandemic
During the covid era, the UK Vaccine Benefit Risk Expert Working Group met regularly. But meeting minutes from that time have only recently appeared:

It is worth noting that:
The minutes published cover the ten months from August 2020 to May 2021, but the minutes from meetings from the subsequent two years remain unpublished, more than 18 months after the last of those meetings.
Some “commercially sensitive information” has been redacted. I am reminded of the recent statement of UKHSA Chief Executive Jenny Harries in the What are they hiding? post.
Minutes of the 27th November 2020 meeting
The minutes reveal that, in the words of pathologist Dr Clare Craig, they knew the issues with the vaccines but ignored them. I have taken the liberty of reproducing her comments, which are the most incisive I have seen:
On 27th November they briefly discussed a lack of any potential benefit for the under 50s but quickly concluded that there was a favourable risk/benefit for anyone aged over 16 years! (link)

They made the case that the already infected should be injected because of lack of evidence of risk!
What about the fact they didn’t need it!? (link)
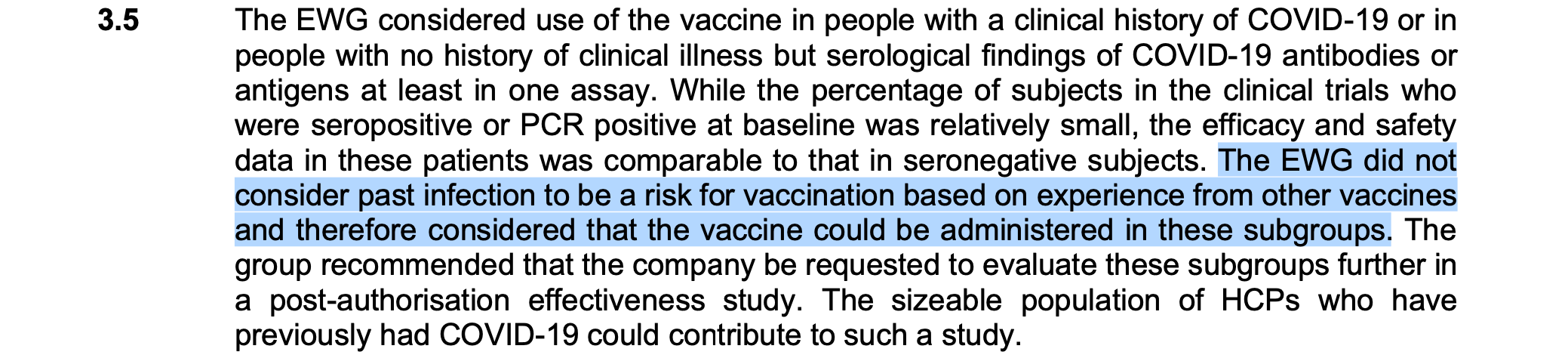
HCP = healthcare provider
They noted issues with early batches. (link)

These were [mass-produced] process 2 batches — not the bespoke process 1 batches given in the trial.
“it is not currently feasible to compare these two batches to those given to subjects in clinical studies.” (link)

The difference between Process 1 and Process 2 batches is described e.g. here:

“it may be the case that the batches the FDA are evaluating are further along the development lifecycle than those allocated for the UK.” (link)

The meeting ended with a reminder to put profits ahead of public health… (link)

I did not find any mention of the possibility that potential longer-term safety risks were considered.
Minutes of the 28th November 2020 meeting
The Expert Working Group reconvened on the following day.
That evening they were told that they were to assess [the] worse batches.
For one they noted visible particulate matter in the vials.
They noted that another had degraded mRNA. (link)

The batch with floaters in it was the infamous EJ0553.1
This was used in the trial resulting in a 13 fold higher incidence of lymphadenopathy… (link)

These were “rejected vials” and they had not done a potency test. (link)

AQL = acceptable quality limit
Don’t worry — the particles “disappear after the product is diluted”!
Also they “were not understood to be associated with a change in concentration of RNA containing LNPs” — but no measurement to confirm this! (link)


It was a problem at the “end of the filling line” — i.e. it was from the dregs of the barrel. (link)

Nucleic acids clump and lipid nanoparticles float — both could result in a higher concentration of product in the last batches to be filled. (link)
The manufacturer admitted “no IPCs [in-process controls] or visual inspection is performed during the manufacturing process until after filling” (link)

There was no data on the process 2 batch performance in humans and no stability data either - both were extrapolated from process 1 in the trial. (link)

Barely any testing on stability. (link)

And evidence that the RNA was degraded. (link)

They ended with a request for more data on the particles. (link)

Three days later Lord Bethell signed off on the drug.
A week after that injections began. (link)
That is the same Lord Bethell who stated, in a written Parliamentary answer in October 2020, at least six months after covid PCR testing had been introduced, that “the United Kingdom operational false positive rate [for the PCR test] is unknown”.
Minutes of the 7th December 2020 meeting
They reconvened on 7th December — the day before injections began.
PHE [Public Health England] were looking at serology (antibody levels in blood) in individuals that “have been vaccinated.” Who are these people injected before 8th December? (link)

They had not had the answers they requested on stability.
They detail all the issues then say — let’s release the batches! (link)


What on earth is redacted here? (link)

The rest of the minutes that day were about AZ and Moderna.
No further comment about the Pfizer batches that were going to be injected into people from the next day. (link)
Minutes of the 10th December meeting
On 10th December:
Distribution was acknowledged as being all over the body. (link)

I presume that the above rat distribution study was the one discussed here in this post:

Or a very similar one. Either way, it had been established that the vaccine lipid nanoparticles accumulated in the ovaries, which was entirely predictable based on the scientific literature.
The vaccine designers would have known that this would happen. And in December 2020 the UK Expert Working Group knew that it was happening.
Minutes of the 17th December 2020 meeting
And on 17th December:
The RNA was worse than the CT = clinical trial batches.
The batches in use had a “higher potency”. (link)


I too wonder what the redacted parts say, and also what the not-yet-published minutes will say.
A partial answer to the latter lies in further minutes also made available recently.
Minutes re the covid vaccination of children (obtained by a Freedom of Information request)
Remarkably, despite the stated “ongoing mission to improve transparency” — Sir Humphrey Appleby would surely be proud — the minutes of meetings held after May 2021 remain unpublished at the end of 2024, more than three years later.2
A Freedom of Information request
But UsForThem — whose video from Molly Kingsley was the subject of the recent What are they hiding? post — have, via by a Freedom of Information request, obtained minutes from meetings held on 6th and 7th September 2021.
They can be found here:

NB it is necessary to click on the arrows (circled) to scroll through the document.
Here is UsForThem’s summary post:

Which also features another video explaining the issues:

The context
The context of the JCVI advice
For context, these minutes relate to early September 2021, when the four UK Chief Medical Officers decided to push ahead with the mass covid vaccination of 12-15-year-olds, despite the fact that the Joint Committee on Vaccination and Immunisation (JCVI) had declined to authorise a mass vaccine rollout.
Here is the JCVI’s advice in July 2021:

The part in the grey box above reminds me of this cartoon:

By mid-2021, it had long been well-established that whatever respiratory viruses were circulating posed essentially zero risk to healthy children.
Here is what the JCVI said in a statement published on 3rd September:3

But in this 13th September letter — which quotes the above paragraph — the four UK Chief Medical Officers (CMOs) wrote to Health Ministers essentially to overrule the JCVI on the basis of “reducing educational disruption”:

Here is England’s CMO Chris Whitty’s statement at the time:
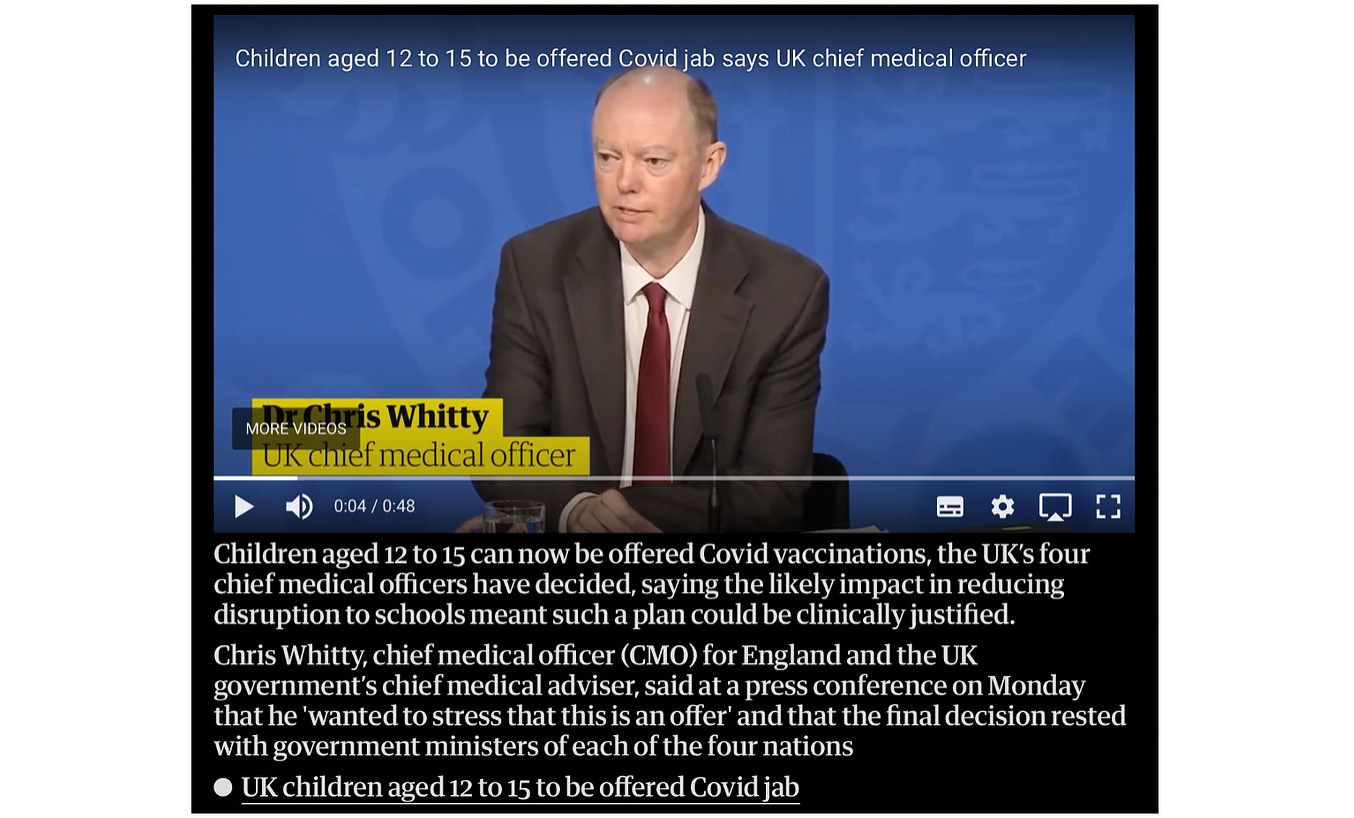
And here is how the BBC covered the decision:

The context of dubious modelling
But the case for “reducing educational disruption” was based on dubious modelling, and ignored other factors, as discussed in this 15th September article from David Paton, a UK Professor of Industrial Economics:

Paton took issue with the modelling paper that estimated “that vaccinating 60 per cent of 12 to 15-year-olds would prevent the loss of about 110,000 days of school in the six months between October and March 2022.”
He pointed out that those 110,000 days equated to:
41 days per thousand pupils or, put another way, just 15 minutes per child.
Over six months.
And added:
To put that into context, if the government had ended the schools’ lockdown just a day earlier back in March, children would have got a benefit 25 times more than that estimated from vaccinating over one million 12 to 15-year-olds.
He also raised other questions about doubtful assumptions used for the modelling, which did not take into account natural immunity from previous infection. And pointed out that the time required for pupils to wait for and receive the vaccine, plus take the recommended 15 minutes rest time…
…would more than wipe out the estimated 15 minutes lost education prevented.
And added that Professor Robert Dingwall, formerly a JCVI member, had pointed out that:
…another 15 to 20 minutes per child would be necessary to establish that their consent is free and informed.
And that:
…the modelling [ignored] any lost education due to vaccine side effects.
But that was not all.
There was other important context based not on modelling but on real world data.
The context of the Pfizer rat distribution study (or similar)
As noted in the first half of this post, in relation to the December 2020 minutes of the UK government Vaccine Benefit Risk Expert Working Group, there was the context of the Pfizer rat distribution study. It was known [see p21 at the link] that the lipid nanoparticles of the Pfizer-BioNTech product could reasonably be expected to distributed all over the body, including to the ovaries of girls receiving covid injections.
As pathologist Dr Clare Craig put it here in this post:

In contrast [to virus spike] the vaccine spike is systemic from the outset. Although people were told it would remain in the arm that could never have been true...
[Consider] EpiPens [which] are given into muscle to quickly get adrenaline throughout the body to treat anaphylaxis. This shows just how ridiculous the claim [is] that an injection into muscle will stay in the muscle… Pfizer-BioNTech clinical trial documents revealed that LNPs travelled to many organs in rat biodistribution studies [that show where in the (rat’s) body the LNPs end up]. Measurement stopped after 48 hours despite signs of an increasing rate of accumulation in the ovaries, liver, adrenal gland and spleen.
The context of warnings about myocarditis
And there were also credible warnings about myocarditis, a serious condition involving inflammation of the heart muscle.4
The Health Advisory & Recovery Team (HART) — a group of highly qualified UK doctors, scientists, economists, psychologists and other academic experts — had written this piece in August in the context of covid injections being offered to 16- and 17-year-olds:

They warned:
The roll out of the COVID-19 vaccine to adolescents has begun, following the announcement on 4 August by the Joint Committee on Vaccination and Immunisation (JCVI) that all 16 and 17 year olds should be offered their first dose of the Pfizer-BioNTech vaccine, despite evidence that myocarditis is a real and serious side effect of the vaccine.
The best real world data, from the Israeli health department, shows a myocarditis risk to young men aged 20-24 after the second dose of Pfizer of 1 in 10,463, rising to 1 in 6,230 for 16-19s, occurring mostly within the first 7 days post vaccination. These figures only include children presenting to hospital. Reflecting the JCVI’s acknowledgement of the risk, 16-17 year-olds are only being offered one dose in the first instance, yet all 18-25 year olds continue to be offered a second dose.
It has been suggested that vaccination in this young age group is valid, as myocarditis can also occur with COVID-19 infection with one non-peer-reviewed paper, using data extracted from health records to show that myocarditis occurred in 0.09% of boys aged 12-19, within 90 days of a COVID-19 diagnosis. However, that estimated rate of myocarditis assumes all cases of COVID-19 are held within their data system, which is highly unlikely to be the case given children are likely to be asymptomatic or with very mild symptoms.
And yet the UK’s four CMOs chose to approve the covid injections for 12-15-year olds. Meanwhile, it appears that those on the Expert Working Group stayed quiet.
Reflections on what the minutes say
Scepticism
In the video mentioned earlier [5:41ff], Molly Kingsley summarises the situation in September 2021:
Whilst [the JCVI] did decline to recommend a mass rollout, within that same meeting [they] effectively passed the buck to the Chief Medical Officers of the UK. And what the JCVI said is, “Well look, we’ve made a clinical recommendation made a clinical recommendation, but, CMOs, if you want to look at broader factors and come to a different view, then go ahead.”
And, unsurprisingly… when the CMOs met — that is the meeting we have the minutes for here… they did make a different decision.
She then turns to the minutes obtained by the Freedom of Information request, and points out that there is nuance in the minutes that is not reflected in published advice. For example, Scotland’s Deputy Chief Medical Officer expressed scepticism about the modelling, and said that the risk of myocarditis need to be taken into account:

Informed consent
[8:43ff] She also notes that the minutes include a statement that a clear informed consent programme would be essential, and that it was important for this to be communicated clearly:

But this did not happen.
She cites this 20th September NHS press release:

Which features this statement from Dr Nikki Kanani, GP and Deputy Lead for the NHS covid vaccination programme:
Alongside one of our busiest summers, NHS staff have been working closely with schools to ensure they are ready to deliver the vaccine to children aged 12 to 15 who are now eligible.
Following the decision by government, and building on the success of the NHS COVID-19 vaccination programme which has delivered over 77 million vaccinations, the NHS will now roll out to hundreds of schools over the next few days.
The vaccine is safe and effective and I would urge families to work closely with their schools based vaccination team to get their loved ones vaccinated when they are invited to protect themselves and their families ahead of the winter period.
And a comment from schoolboy Jack Lane, 14, one of the first to be vaccinated in England, as part of the extended rollout:
I am proud to have had my vaccination so that I can remain in school and continue in my education — the jab was quick, easy, and painless.
Kingsley asks:
Where is the nuance? Where does it come across that this is a finely balanced decision? Where is the mention of risk? There is none.
And in December, the Department of Education’s messaging looked more like advertising than objective public health information based on robust science:

As Kingsley notes:
There was no mention of natural immunity, which was known to be superior even then. And there was no mention of risk.
She asks how it was possibly thought that this was going to be:
…a programme that could be given in compliance with principles of truly informed voluntary consent.
And notes that in Autumn 2021:
…the vaccine rollout had taken a deeply sinister and coercive turn… in the UK we had vaccine passports being needed for travel… a semi-coercive measure to increase vaccine uptake including in children. And then… the care home mandate and so on…
She then highlights independent polling of a nationally representative sample of over 2000 people:
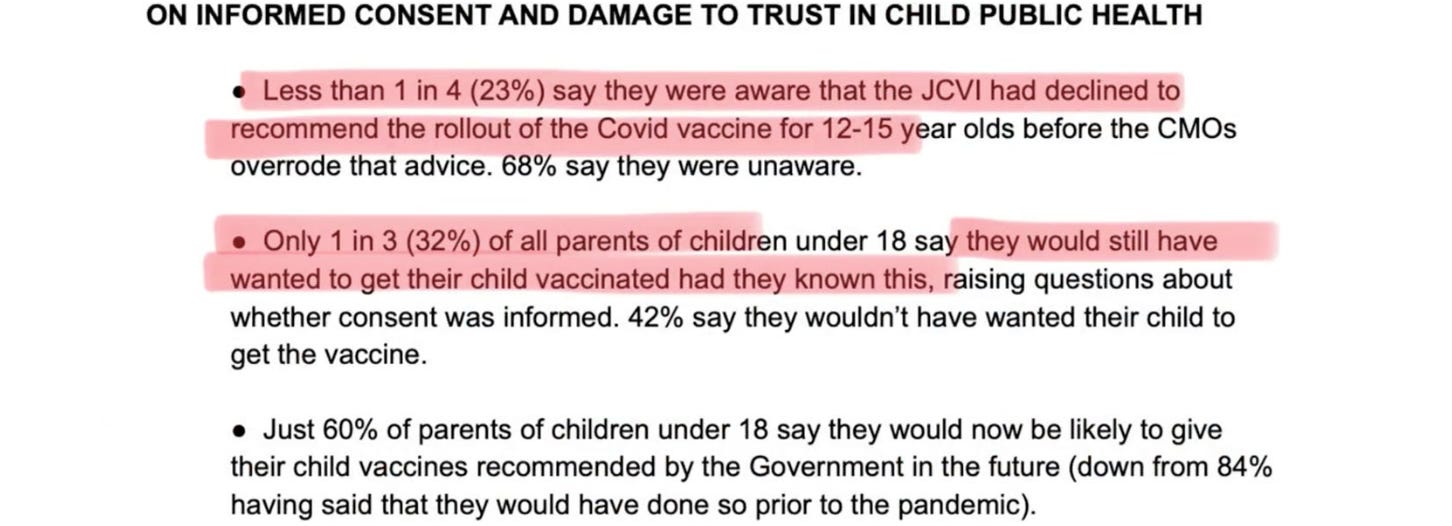
And notes that the polling:
…was offered across all [mainstream] print media, and no-one wanted to publish it.
Reflections on what the minutes do not say
Kingsley then turns her attention to the matter of what the minutes do not say — which is also revealing.
Conflicts of interest
[12:32] She discusses the issue of conflicts of interest, and notes that the fact that the Royal College of General Practitioners (RCGP) received almost £49,0005 from Pfizer in 2020 was not recorded in the minutes:

And yet the minutes do record that the RCGP strongly endorsed covid injections for children:

The shutting down of the UK government’s ethics committee
[16:49] But what is perhaps the most shocking thing about the discussion around covid injections for children is the lack of mention of ethics.
Kingsley points out that, during the pandemic, there was actually a specialist ethics committee called MEAG — the Moral and Ethical Advisory Group.

Kingsley comments that the MEAG…
…predated the pandemic, but advising on pandemic matters was very surely within its remit. And… for the first year or so of the pandemic, it did advise on pandemic matters. It had met weekly. And it had set out its intention to advise on childhood vaccination against covid. And, as the time came nearer for that… in the run-up to late summer 2021… it did start advising on that. And the… all-expert committee [made it] clear that they had serious concerns about vaccinating kids on the basis that the vaccines were invasive, irreversible and may have long-term side-effects. And they put those concerns in writing.
However, before the concerns could be formally discussed with the Department for Health or with the CMOs, the committee were sent on what can only be really described as an extended sabbatical.
There had been a meeting in June 2021 that was due to be held, talking specifically about… the many ethical issues involved in vaccinating kids. The meeting got cancelled at short notice, the day before it was due to be held… And the group were not convened until — quite shockingly — the day after the CMOs had made their decision… to push ahead with the vaccination of kids on 7th September… It is not clear whether any ethical input was sought by the CMOs or received…
MEAG were not reconvened until 8th September, and, unbelievably, when they were… reconvened, they were not allowed to talk about kids’ vaccination against covid. MEAG were only allowed to talk about issues that they had been asked to advise on. And on this occasion… the day after possibly the most ethically contentious decision of the entire pandemic, they were asked to advise on virginity testing.
MEAG limped on for a few months after that… but they were never again asked or allowed to advise and input on pandemic or vaccination-related topics.
For more details, see e.g. this article:

Questions and concluding thoughts
Ethical questions
[21:26] Kingsley asks:
Whose decision was it to disband the ethics committee at this moment of critical ethical jeopardy for children? Why were they not reconvened? Was it an act of choice? Was it an accident?
Was the committee’s strongly-stated concern about the vaccination of children a factor in that?
What ethical input was sought… and received by the CMOs before they decided to overturn the government’s own vaccine advisers and push ahead with the vaccination for covid.
And then concludes with two further strands of thought.
The “workaround”
[22:07] She points out that it appears that the JCVI was never overridden before before 2021, and has not been overridden since:
It seems to be absolutely unprecedented and really quite unorthodox. Yet if you listen to what Chris Whitty had to say about it back in 2021, you might be mistaken for thinking it was a… more normal occurrence.
Giving evidence in front of the Education Select Committee in September 2021 after the JCVI override, Whitty… said that in the situation where MHRA have authorised a vaccine but JCVI have declined to authorise it to the population, “the CMOs are kind of third umpire”

She adds:
We can’t find another instance of it happening. Nor can we see any documentation anywhere that it was even envisaged it might happen. And I think we might question whether Whitty’s description of that override to the Select Committee perhaps suggests a degree of normalcy which wasn’t reflected by previous events.
She adds that, in a meeting of the Science and Technology Committee later that year, in December, Jeremy Hunt, Chair of the Committee at the time:
…candidly described the CMOs’ recommendation as a “workaround”

The covid inquiry
[24:05] She asks:
Where is the covid inquiry in all of this? These were really serious issues. And many of us have been left very shaken by what happened in 2021. We are seeing now the knock-on impact in terms of lack of trust in public health and, in particular, childhood immunisations… And yet, as far as we are aware, there has not been a single mention of this desperately unorthodox period of decision-making in the covid inquiry.
And that is very, very odd, because although the module on children is yet to come, we’ve already had the module on high-level decision making... And one would certainly have expected decisions such as this… affecting millions of… children to have been looked at.
Likewise, one would have expected an issue of a disappearing ethics committee to have been picked up. And yet so far we haven’t heard any reference to it…
And she concludes by pointing out that everything that she has said is referenced and footnoted, and points to the details documented in a book — The Accountability Deficit — that she has co-authored:

I await further developments with interest.
Related:




Dear Church Leaders most-read articles
Some posts, including a version of this one, can also be found on Unexpected Turns
The Big Reveal: Christianity carefully considered
See e.g. https://www.gov.uk/government/publications/freedom-of-information-responses-from-the-mhra-week-commencing-11-july-2022/freedom-of-information-request-on-yellow-card-report-data-for-covid-19-vaccines-foi-22775
This letter published in the British Medical Journal around that time, provides further context:
The government has refused to release the minutes of the meeting in which its vaccine advisory committee decided not to recommend vaccinating all 12-15 year olds against covid-19 [according to this Freedom of Information request].
The UK Health Security Agency, which replaced Public Health England, rejected a freedom of information request for the document on the grounds that it intended to publish the minutes “in due course.”
The agency argued that it was in the public interest to withhold the information until it could be released in a “simultaneous, coordinated manner” and that disclosing the minutes before they were finalised could “result in a false impression of the contents of the meeting.” The decision is being appealed.
On 3 September the Joint Committee on Vaccination and Immunisation (JCVI) said that it would not be recommending universal vaccination for 12-15 year olds because although the health benefits of vaccination were “marginally greater than the potential known harms,” the margin of benefit was considered too small. The committee did not explain what factors its conclusion was based on, and neither the minutes nor the data behind the decision have been made public.
The JCVI asked ministers to seek further advice from the UK’s chief medical officers on the wider potential benefits of vaccination. The government later (13 September) accepted the chief medical officers’ recommendation to vaccinate all 12-15 year olds on the basis of an assessment that included transmission in schools and the effect on children’s education.
In a letter dated 5 October academics from Independent SAGE wrote to the JCVI highlighting the fact that, despite the committee’s own policy stating that draft minutes would be published within six weeks of each meeting, the last publicly available minutes were from February 2021.
They urged the JCVI to “abide by its code of practice and be open and transparent through rapid publishing of all agendas, supporting papers and minutes,” arguing that “public confidence in vaccination programmes is assisted by clear and consistent processes and messaging.”
They added, “In that spirit, we wish to have a public assurance from JCVI that all future considerations of covid-19 vaccines, including the extension of vaccination to children under 12 years of age, will be conducted openly and transparently.”
In December 2024, those minutes have still not been published.
NB that paragraph was quoted selectively, i.e. without the comment about margin of benefit being too small, in this BBC Verify article from 14th December 2021

According to this paper, “Myocarditis is an inflammatory disease of the myocardium caused by infectious or non-infectious agents. It can lead to serious short-term and long-term sequalae, such as sudden cardiac death or dilated cardiomyopathy. Due to its heterogenous clinical presentation and disease course, challenging diagnosis and limited evidence for prognostic stratification, myocarditis poses a great challenge to clinicians.”
Via https://www.abpi.org.uk/reputation/disclosure-uk/