


[SPCI-3] "Just from simple first principles, we can understand that these are really harmful measures that were implemented"
Professor of Ecological Genetics Richard Ennos on the expected outcome of covid measures
Dear Church Leaders (and everyone else)
This is post #3 in a series featuring presentations at the recent Scottish People’s Covid Inquiry (SPCI, as distinct from the official Scottish Covid Inquiry).
This one is from Richard Ennos, Professor of Ecological Genetics and now Honorary Fellow at the University of Edinburgh, discussing what we might reasonably have expected as the outcome of the covid measures.
I have added occasional additional material in the transcript below.
Responsibility for Scottish covid measures

We’ve already heard from Alan Mordue about the general measures that were taken by the Scottish government in March 2020. And what I want to do is to have a look at those in some detail, and ask the question… what we’d anticipate just using common sense. What would we anticipate to be the effect of these measures on the Scottish public?
Just to remind you… the three graces… First Minister Nicola Sturgeon, Cabinet Secretary for Health and Sport Jeane Freeman, Chief Medical Officer for Scotland — for a time… before she had to resign — Catherine Calderwood… Those are the people responsible for signing the letters which implemented an awful lot of these measures.
Movement of elderly from hospital to care homes
The first measure that they implemented [in] March 2020… movement of the elderly from hospitals to care homes. And from March 1st to the 31st of May 2020, nearly 5,000 discharges were made… into care homes from hospitals. That brought about a 10% increase in the care home population. 50% of those people had never been in the care home before, so it’s a new place that they were sent to. 50% of those places did not have any medical support. So these people who were being taken out of a hospital were being taken to a novel place they’d never been before… many of them had dementia, and in many cases there was no medical care available at those care homes.
There’s a report by the Mental Welfare Commission for Scotland… shows that 20 of these where they’ve looked in detail were actually unlawful. Hundreds more were made without appropriate legal safeguards for these people who… lacked capacity. And in one case there was an internal decision made between the Health Board and… a company of care homes. And that was where the decision was made to move the people. The people themselves were not actually consulted. And no, there’s no… consent of those individuals of the families and or the health and welfare attorneys. There’s a clear breach of Article 5 of the human rights… deprivation of liberty.
Now what would we anticipate — just as people in the general public — to occur as a consequence of this?
Well, we would expect actually that a lot of these people who no longer had medical care — and they were in places where they were understaffed — we would expect an increase in the rate of death of these people. And indeed these people have actually been followed, and, within a month, 1 in 7 of them had died. It’s about 7x the expected rate of death. And by three months, 1 in 4 of them have died — about 4x times the expected death rate. So that’s what we would have anticipated, just as members of the general public understanding about how you look after elderly people.
Here is a chart showing the deaths by week of registration in Scotland before and after lockdown:
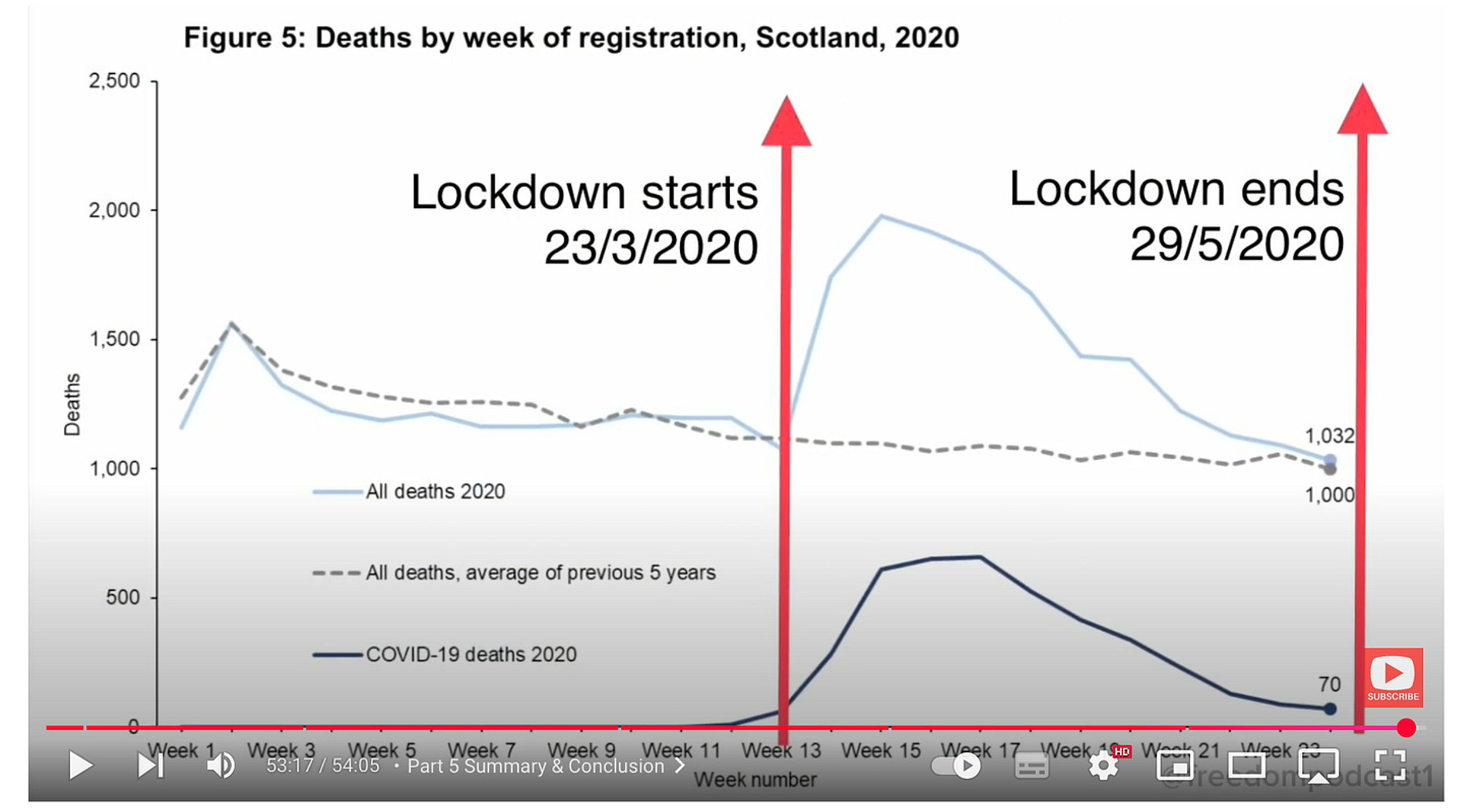
It’s worth taking stock of the left-hand side of that graph, which shows that the death rate before lockdown started was at normal levels for the time of year.
For context, covid had reportedly been circulating in the UK since at least the end of January (week 5).
The pattern is very similar in England and Wales, according to figures from the ONS featured in this post:

It is in stark contrast to e.g. 2018, when the excess deaths figure for England and Wales was around 50,000 as discussed here:

And yet I do not recall anyone suggesting in 2018 that we should do anything out of the ordinary…
Cessation of visits to, and extreme isolation within care homes

The second thing that was done was that there was a cessation of visits, and extreme isolation placed on people who were in care homes. In a care home there’s usually ongoing medical treatment that people receive, and recreation… social support to enliven their lives. People not going into care homes meant there was no scrutiny of what happens… My mother-in-law is in a care home at the moment, and I understand how important it is for families to go in and see that their loved ones are being looked after properly. That was taken away. There was no scrutiny of what was going on in those care homes.
Often people were confined to their rooms… virtual solitary confinement for 14 days. And all of the emotional and practical support provided by families was totally cut off from those people in care homes. And often their routines — which are incredibly important if you have dementia… routine is really critical — that was destroyed. And what would we expect? A rapid decline in the physical and mental health of those people, and a huge increase in death rate. So just from simple first principles, we can understand that these are really harmful measures that were implemented.
Change to medical certification of cause of death

What else happened? Well, there were changes to the way in which medical certification of cause of death was put in place... complete reduction in rigour. All that was needed at these times was that the doctor had to [have] seen the patient remotely, within the last 28 days. They didn’t have to see them in person… to sign a medical death certificate.
These are some quotes: “Covid-19 causation is acceptable if the patient has displayed symptoms consistent with covid-19” — which is if they had a cold or a flu.
And covid-19 causation is acceptable if you recorded a positive result — a non-diagnostic test as I’ve explained [in part 1 of this series] — within 28 days of death. So what would you expect? A massive inflation of so-called “covid deaths”. And actually a massive reduction in deaths from other causes, because people were dying of something else but they were put down as “dying from covid”.
And I know this from personal experience, because my father... he was dying from heart failure, and… he was in hospital... two days before he died... they tested him... he had a positive test for covid. On his death certificate, it says he died of covid pneumonia. He didn’t die of covid pneumonia at all. He died of heart failure. So that’s just one instance, but this is repeated over and over and over again.
Use of DNACPR (Do Not Attempt CardioPulmonary Resuscitation) forms

The next thing that was done was inappropriate use of the “Do Not Resuscitate” (DNR) forms. If used properly, these are very good, because if you’ve got somebody at the end of their [life] they’re very frail. You don’t want to be going pounding their chest at the end of their life. It’s incredibly undignified, and it could break their ribs and things like that. So it’s a good thing to have such forms to say [that] when somebody is at the end of their life we shouldn’t attempt resuscitation. We should just let them die.
In order to apply these forms, it requires the individual consent, or that of a power of attorney. And it doesn’t have any implications for any other treatments that person is undergoing. So they would be treated normally for other other conditions.
What happened during this period is that there was blanket application of these forms to all residents in a care home in some instances. Cold calls were made by GPs to people who had certain disabilities, and people were asked, “Do you want have a DNR form?”... a cold call about such a sensitive issue… This is incredible.
Often no consent was given, and people found out that their relatives had one of these forms associated with them. And in some cases those signatures on those forms had actually been forged. The other really important thing to understand is that, if you had a DNR notice on you, then that was used to deny access from a care home into a hospital. So if the ambulance came and they found that they had a DNR form on the person, then they wouldn’t take them to the hospital. Consultants refused to accept people at the hospital.
And those people in hospital who were required to go to the ICU... they were denied access because they had a “Do Not Resuscitate” form on them. So it was used in a completely inappropriate way.
And what would we expect as a consequence of this? Well, people would be denied care which they would normally have — and they would have survived — but in this case they didn’t have that care, and they died. So we would expect this use of the forms in this way would increase the rate of death of people, particularly in care homes and hospitals.
Medical protocols following covid diagnosis
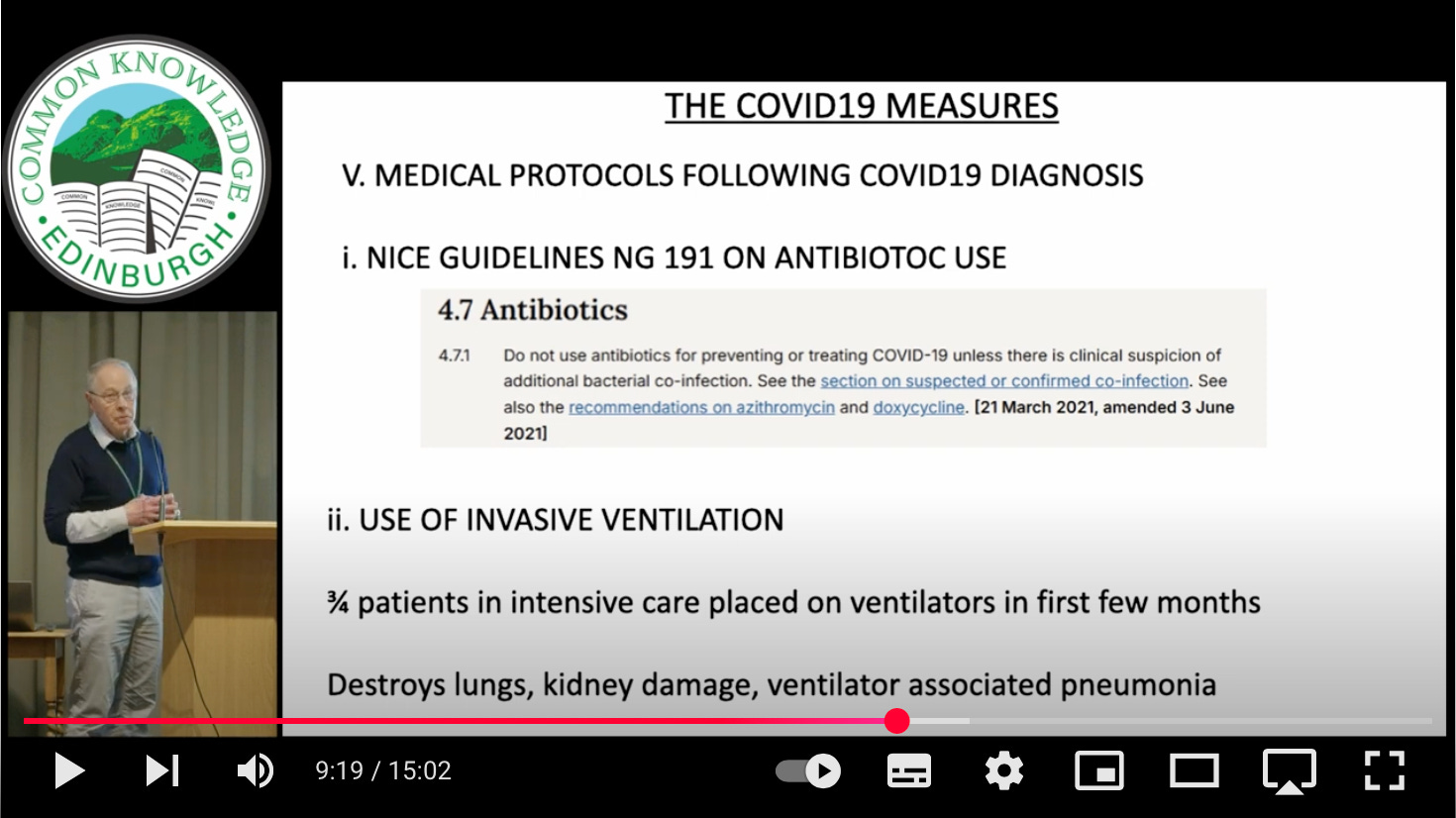
The next thing that we should talk about has already been mentioned... is medical protocols which were adopted during this time.
The first one is one which is about antibiotics: do not use antibiotics for preventing or treating covid-19. Normally, if somebody was to have a respiratory disease, you might prophylactically give them antibiotics to prevent them getting bacterial pneumonia. Well, that was denied [to] people who were designated as being covid-19.
Here is the data from OpenPrescribing, which shows NHS prescriptions in England:

In contrast to the peaks in the winters of 2019/2020, 2021/2022 and 2022/2023 (and to a lesser extent 2023/2024), the number of prescriptions for antibiotics was remarkably low during Spring 2020 (the “height of the pandemic”) and Winter 2020/2021.
There was [also] excessive use of ventilation. And from the article in the BMJ, three quarters of patients in intensive care were placed on ventilators in the first few months of the lockdown. And ventilators have to be used with extreme care, because they have the capacity to just destroy people’s lungs and their kidneys and lead to so-called ventilator-associated pneumonia. So that was going on in hospitals.


There was also enrolment of individuals into experimental programs which were designed to test what’s the best treatment for covid-19. And here’s one of them — the REMAP-CAP trial. And here the patient would be allocated at random to a particular treatment. They weren’t given a treatment that was appropriate for them. They were part of an experiment. And the kind of treatments are… either you get antibiotics or you don’t. Or you have a powerful immunosuppressant provided, or not. And individuals were randomly allocated to this. And I think we’ll hear later on today that in some cases people were recruited to these trials with forged signatures.
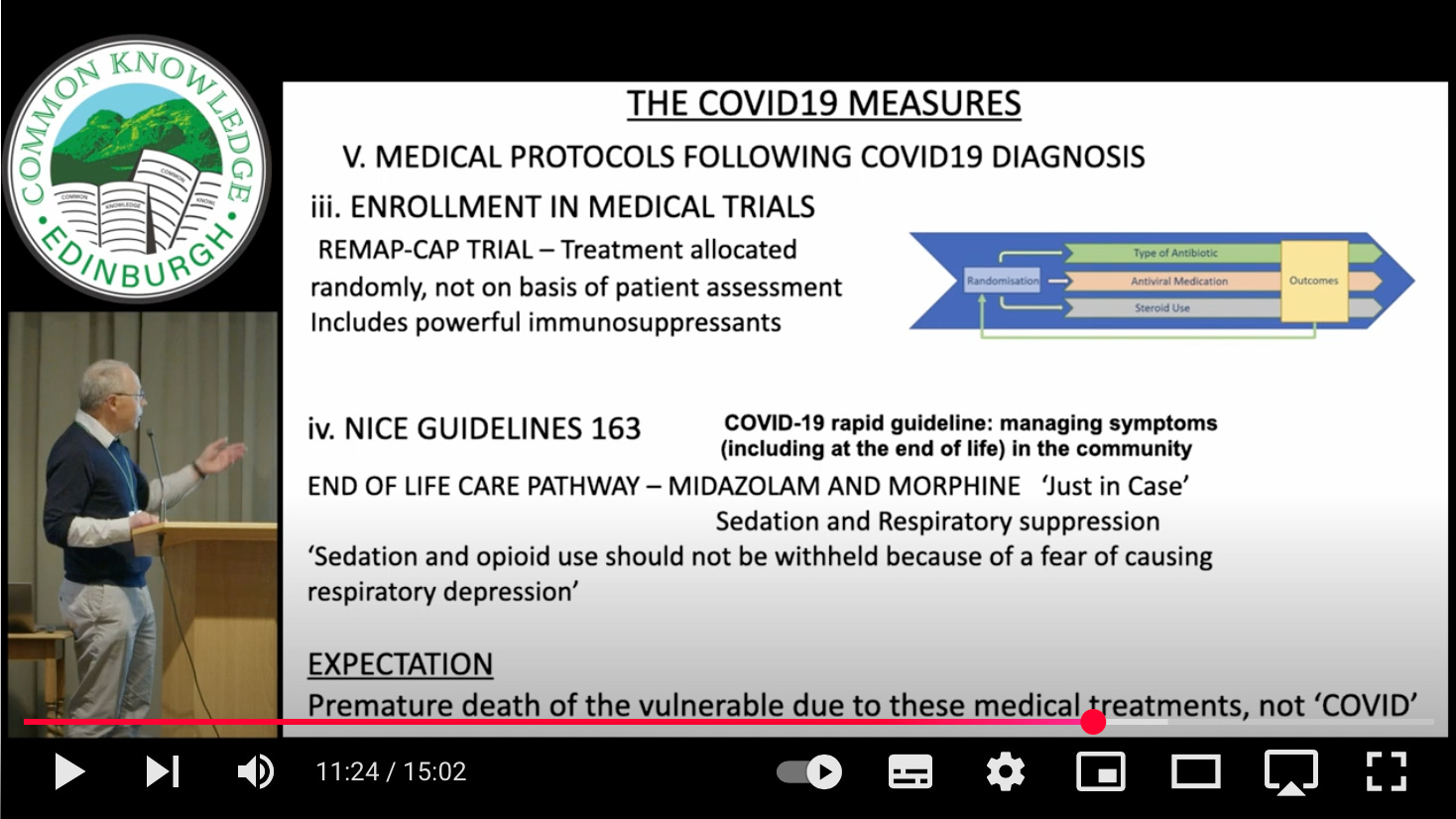
And… the NICE guidelines on end-of-life care... We’ve got the notorious NG163, where people considered at the end of end of life were given midazolam and morphine. And this is was referred to as “just in case” medication. And often all that was required is that the person actually tested positive for covid-19 using the fraudulent tests.
This sedates people, and it causes respiratory suppression, so essentially what you’re condemning people to is a death through asphyxiation. And one of the lines in the protocol says, “Sedation and opioid use should not be withheld because of a fear of causing respiratory depression.” Okay, so go ahead, don’t worry about it…
The document NG163, COVID-19 rapid guideline: managing symptoms (including at the end of life) in the community, which is no longer available on the NICE website, but can be viewed e.g. here (archived version) or here (pdf, c/o this related article):

So what would we expect? Well, we would expect premature death of those vulnerable people who had been put on these pathways.
Criminal investigation of care home staff

And the last thing I wanted to mention is that another measure that was taken… of course.. there was an enormous death in care homes at the beginning after the lockdown happened, and some 6,000 were ascribed to covid-19 in care homes from March to May 2020.
What was the government’s response to that? The government’s response to that was not to investigate why this occurred, but to start a criminal investigation of deaths by the Crown Office in 2020… but no similar investigation of deaths in the NHS at that time. So care home staff came under scrutiny and became traumatised during 2020 by the ongoing — and it is still an ongoing threat — of prosecution.
So what would we expect? Well, we expect as a consequence of that that they would then be very keen on adhering to any government regulations, because if they went out with that then they’re going to be in trouble when they come around and Operation Koper comes and has a look at what they’ve been doing.
Here are comments from January 2021 from Scottish Care, which represents around 350 organisations, which totals almost 900 individual services, delivering residential care, nursing care, day care, care at home and housing support services:

Political exploitation of the care home deaths

So, just a reminder... there’s enormous care home deaths. How did it [get] used politically? These deaths are used politically to say that covid is a really serious disease, because all these people are dying of it. And we know who did that.
Anticipated effects of covid measurements taken by the Scottish government
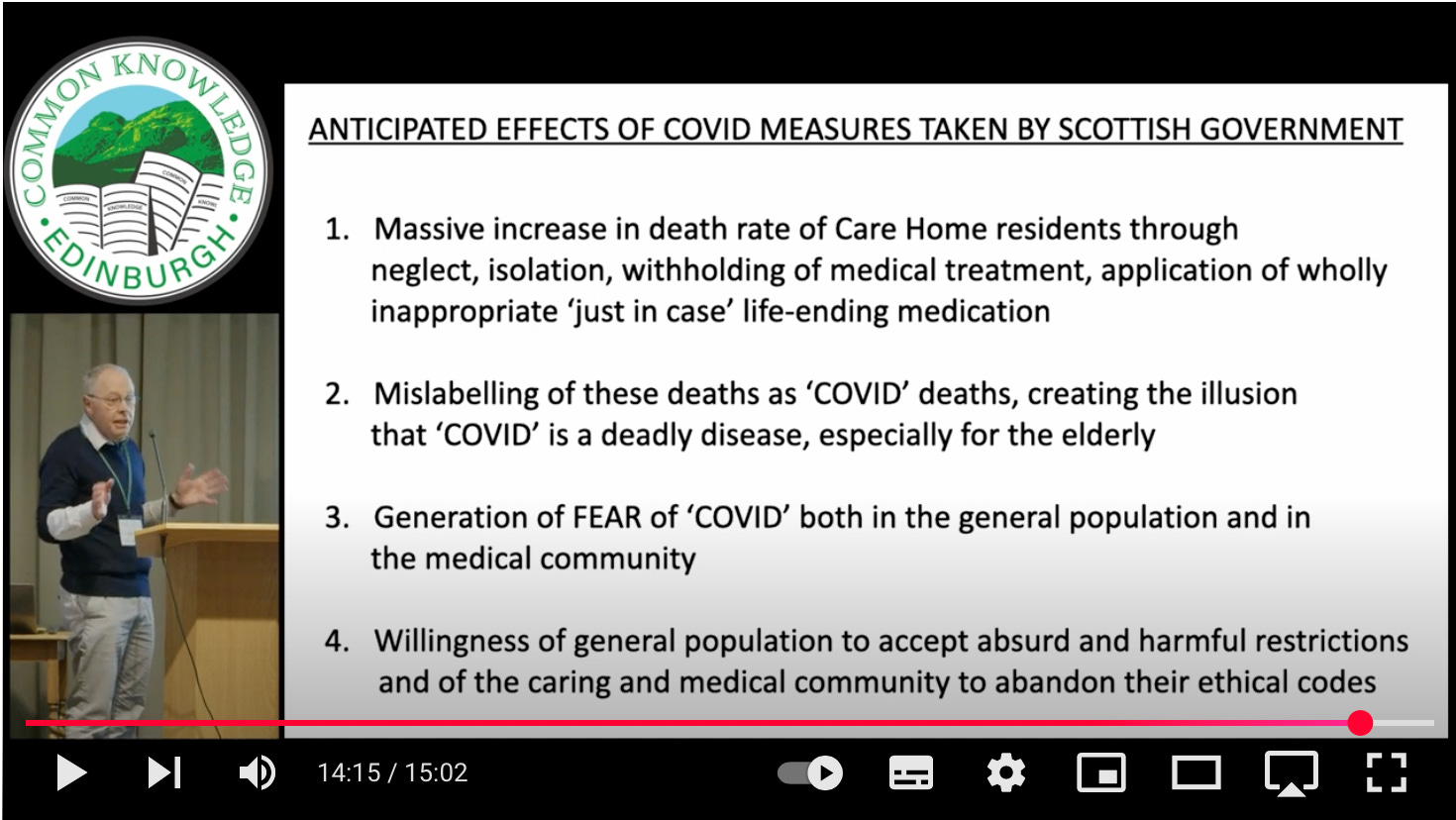
So what are the anticipated effects of all these measures that were put in place by the Scottish government?
Massive increase in death in care homes through neglect, through isolation, withholding of medical treatment, application of inappropriate “just in case” life-ending medication.
Mislabelling of these deaths as covid deaths, creating the illusion that covid is a deadly disease, especially for the elderly.
And then the generation of fear of covid in the general population and the medical community.
And I think that to a large extent accounts for the willingness of the general population to accept absolutely absurd and harmful restrictions, and those in the caring community and the medical community to abandon a lot of their ethical codes.
There are of course many parallels to the above in England and Wales and other countries.
Related:


And these highlights from the official Scottish Covid Inquiry:
Links to the other posts in the series:
#1 Alan Mordue | #2 Diane Rasmussen McAdie | #3 Richard Ennos | #4 Alison Walker
#5 Pam Thomas | #6 Bill Jolly | #7 Martin Neil | #8 Liz Evans | #9 Clare Craig
Dear Church Leaders most-read articles
Some posts, including a version of this one, can also be found on Unexpected Turns
The Big Reveal: Christianity carefully considered as the solution to a problem