
A courageous cardiologist
“If I don’t do this, who is going to do it…? Someone has to stand up for the truth...”
Dear Church Leaders (and everyone else)
This posts features the story of Dean Patterson, a leading consultant cardiologist in Guernsey and Fellow of the Royal College of Physicians.
In early 2024, Dr Patterson wrote to the GMC (General Medical Council) in support of fellow cardiologist Dr Aseem Malhotra, who had spoken out in the context of covid vaccine harms.
According to this March 2026 article in the Guernsey Press:
[Dr Patterson] has had his medical licence suspended by the General Medical Council [GMC] and is no longer a partner at the Medical Specialist Group [MSG].
He had not been involved in patient care since February 2025 and ceased to be a partner at the MSG [in March 2026], the group said in a statement issued in response to Guernsey Press questions, the newspaper having discovered the GMC’s suspension of his licence last month…
[The MSG] confirmed that [in February 2026] the General Medical Council imposed a 12-month suspension of Dr Patterson’s medical licence as an interim order pending the outcome of fitness to practice proceedings relating to him. Dr Patterson is appealing this suspension.
‘The investigation by the GMC is ongoing, and it is important that this process is allowed to run its proper course,’ said the MSG.
‘Separately from those GMC proceedings, following the conclusion of our internal processes, we can confirm that as of 19 March, Dr Patterson is no longer a partner at the Medical Specialist Group.’
“The process is the punishment.”
Prior to the above recent developments, Dr Patterson told his story here in conversation with orthopaedic surgeon-turned-podcaster Doc Ahmad Malik:

It is a fairly long podcast, and the transcript below — of the most salient parts, plus occasional links and comments — makes for a lengthier post than usual. But it is, I think, worthwhile.
Background
[Doc Malik] Dean Patterson… I think you’ve got a lot of interesting things to say… tell me a little bit about yourself…
[Dr Patterson] …I’m based in Guernsey… a Channel island… about 80 miles south of Southampton… a crown dependency… a… unique legal disposition in terms of… part of the UK… population 65,000…
I was born in South Africa and I [did] my medical degree there… I left in [the 1990s]… I… worked in Cheltenham [in England]… and then I went to Scotland. I trained in cardiology and vascular medicine [and] did some research in cardiovascular therapeutics [where] I saw quite blatantly how pharma was calling the shots… when the big drug companies were involved, the data was… held by the drug companies… ghostwriting was taken for granted… the system is not set up right….
I was looking to possibly head to Australia… and found in the career section an advert for Guernsey. So I came here. And I’ve enjoyed it. It’s been really tough. It’s a sort of hybrid system where we work as a partnership. [And on that note] these views that I’m expressing are my own… they don’t represent the partnership. I’ve been asked to say that by the management of the partnership.
We have a contract with the state of Guernsey and we provide secondary healthcare services… apart from radiology, psychiatry and pathology… about 50 specialists. I was a cardiologist on my own from 2006 to 2016, and then we recruited another colleague. [And] I’ve just been doing what I’ve been normally doing… listening to my patients.
I pride myself as being a very ethical diagnostician. I stick to what I call classical medicine in terms of… the history tells us nigh on everything that we need to know to make a diagnosis. And that’s all I’ve been doing… when I entered this covid situation… I was just following my standard principles…
Wisdom is something that you accrue over time and you never stop learning. But… when you get to a certain age and… level of experience, you know, in your heart… in your gut… you know absolutely when you have something that is on the money… that there’s a problem.
Spring 2021 observations
And I noticed [in Spring 2021] one of my patients [with] heart disease… admitted with an acute coronary syndrome… chest pain… he was admitted by a colleague [and] I took… over [his case] the next day.
I knew him really well and… I said to him, “How are you feeling today?” He was feeling a lot better, and I had a look through his notes… and I said, “This is really interesting… you were here in October last year… 2020… you [had investigations] in Southampton and they couldn’t find anything wrong with you… and you look like you’re having exactly a replica of [what happened last year]…” [So] I said, “What do you think is triggering this…? What’s been going on?”
He said, “I’ve actually been fine between these two events… [and] actually, Doc, the only thing I can think of is the fact that… five days before my admission in October last year I had my flu vaccine… and I’ve had my covid vaccine seven days before this admission [in Spring 2021]”.
[Doc Malik] Wow…
[Dr Patterson] And that was the first point where I actually thought… ever in my life… that a vaccine could do something to any of my patients. It wasn’t something against covid. It was really just listening to the patient…. You bury it in the back of your head and you think, “Okay, maybe he’s got a point.” He set it down… we managed it medially… he’d been thoroughly investigated on many occasions so he wasn’t keen on having further investigations… he was known to have had reasonably complex coronary disease, but… he was living quite a good quality of life apart from those two episodes… I followed him up subsequently…
But… it was literally a week later… another patient was… admitted within 24 hours [of a vaccine] with chest pain… And then a week later I had [a] patient who was probably one of the worst sort of coronary patients… diabetic… poorly controlled… [had] not really looked after himself… had a bypass and was… not expected to do that well… but he was in his sixties… he was admitted, and he collapsed… and he was in intensive care…. we weren’t sure what it was… [And] I’ve gradually got [more and more of these instances] of people getting admitted with… cardiovascular collapse and odd things that didn’t quite fit.
And then one of my patients [who] I’d been seeing for 10 years… she went to the emergency department and she’d become breathless within a week of her first jab… I knew her well because she had a previous [episode of heart trouble]… about 10 years before. But she [had been fine since]… no previous admissions apart from the one ten years before… when she was [first] diagnosed…
I had a look at her… we investigated… her breathlessness… and my gut told me that there was something going on… and I just couldn’t… figure out what it was in this particular instance… because she had a complex previous history… she was on [anti-clotting] medication. And then she got a second shot… she was in [intensive care] and she collapsed with cardiogenic shock [when your heart cannot pump enough blood and oxygen to the brain and other vital organs] and she passed away…
At that point I thought to myself… “There’s definitely something brewing here… And I had to stand up for myself… for the first time ever… I’ve never in my life had to stand up and say, “Look, I want a post-mortem…” She was in her 40s. She was stable in my care for 10 years. I knew her. She relied on me. And I felt that we had let her down. And I had to stand my ground. And I said to the pathologist, “Look, I want a post-mortem. I’m not backing down.” And everybody was trying to tell me, “Don’t push for a post-mortem…” my colleagues... I felt the pressure… people were saying, “This is unnecessary.”
[Doc Malik] Why? Why is it unnecessary?
[Dr Patterson] Well, they were [making out that it was] just a foregone conclusion… she had medical conditions... a [history of heart problems]. [And that] she died because of her known condition. I said to them, “No, I don’t buy that, because it was a temporal relationship with this vaccination, and she was stable before.” She had been stable for ten years and she never had covid… we had tested it… Also… when patients honour my care, I stand by them. I’m there to protect… if things go wrong, I will do my best to figure out what went wrong and document it. [In] medicine we need to learn through our mistakes… that’s the ultimate judge… if we make an error, we have to actually own up to it.
[Doc Malik] In surgery, we have something where… if you die within 28 days, you’re meant to discuss at an M and M [mortality and morbidity] meeting and have a post-mortem. Does that not exist in the field of cardiology…. where if there’s a medical intervention or something…?
[Dr Patterson] It does… but… I’ve never… formally ever before recommended a post-mortem… I’ve taken advice [when I’ve] asked for post-mortems… when people say, “No, we’ll just leave it.” But in this particular situation I felt strongly enough because of the uniqueness of the patient. She was young [to die]… and she had a youngish daughter. And the fact that she was so stable under my care… and the abruptness of the deterioration… And… these inklings [I had had] before made me think… “Hang on… you can’t let this slide… we have launched this vaccine quite quickly and we don’t have any long-term safety data…”
The post-mortem came back and I got [an] apology from the pathologist… she apologised to me personally and in front of the M and M meeting. The patient had what we call thrombotic endocarditis… basically a [heart] valve being destroyed by [blood clotting]… But on top of that, she had devastating myocarditis [inflammation of the heart muscle]. [The left chamber of her heart] was completely destroyed.
I was at that point picking up some post-mortem findings from... a pathologist from Germany… I got in touch with him and I tied it in with our local pathologist because she wasn’t experiencing all these things. And we managed to try and get some headway on this to find out… is this from the vaccine… how do we diagnose it etc. The post-mortem… against my wishes… stated that they could not exclude covid-19 as a cause for her death… whereas I actually felt that this was… clear… In any other situation where… an intervention had happened… and a patient dies with that temporal relationship… then you have a duty of care to say that this is a probable cause of her death. You don’t say… “unable to exclude [X] as a cause of death”. That’s a real cop-out. So I wasn’t particularly pleased about that.
[Doc Malik] The flip was also true… if you died of even a car crash within 28 days of a covid test, you “died of covid”. So why is the flip not also applicable… where if you die within a week of the jab, it’s likely to be the jab… or it has to be the jab until proven otherwise…
[Dr Patterson] Yes… so that was a moment to… stand up and say, “Actually, there is a problem”, but still a lot of people just saw those patients having chronic disease [as] being unlucky, and they didn’t even want to know whether it was anything to do with the vaccine.
And [then]... I think it was because they started to vaccinate younger people… we had a 20-year-old who was admitted with what we think was [a heart attack]… He first had a little rash and then he started getting this ache in his chest and he was admitted to the hospital… [around] 36 hours after his Pfizer vaccine, and he was in a real state… [the] worst chest pain you could ever think of. He was extremely lucky [to survive]… [and] this [sort of presentation] is something I’ve never seen in my life [before the covid era]…
And… there were two other cases in younger patients… of myocarditis… [in] a population of 63,000. So according to data estimates from the Office for National Statistics, we should be seeing… over a ten year period… two or three hospital admissions with myocarditis and maybe ten [related] cases overall. [But] I had this patient pass away… I had two other patients come to hospital... one… female, another male… in their 30s and 40s… with myocarditis. And then this patient who was 20… with myocarditis.
I am reminded of this UK government data (p18 here) for the most serious ambulance calls shows that the numbers rose substantially during 2021 and continue to remain high:
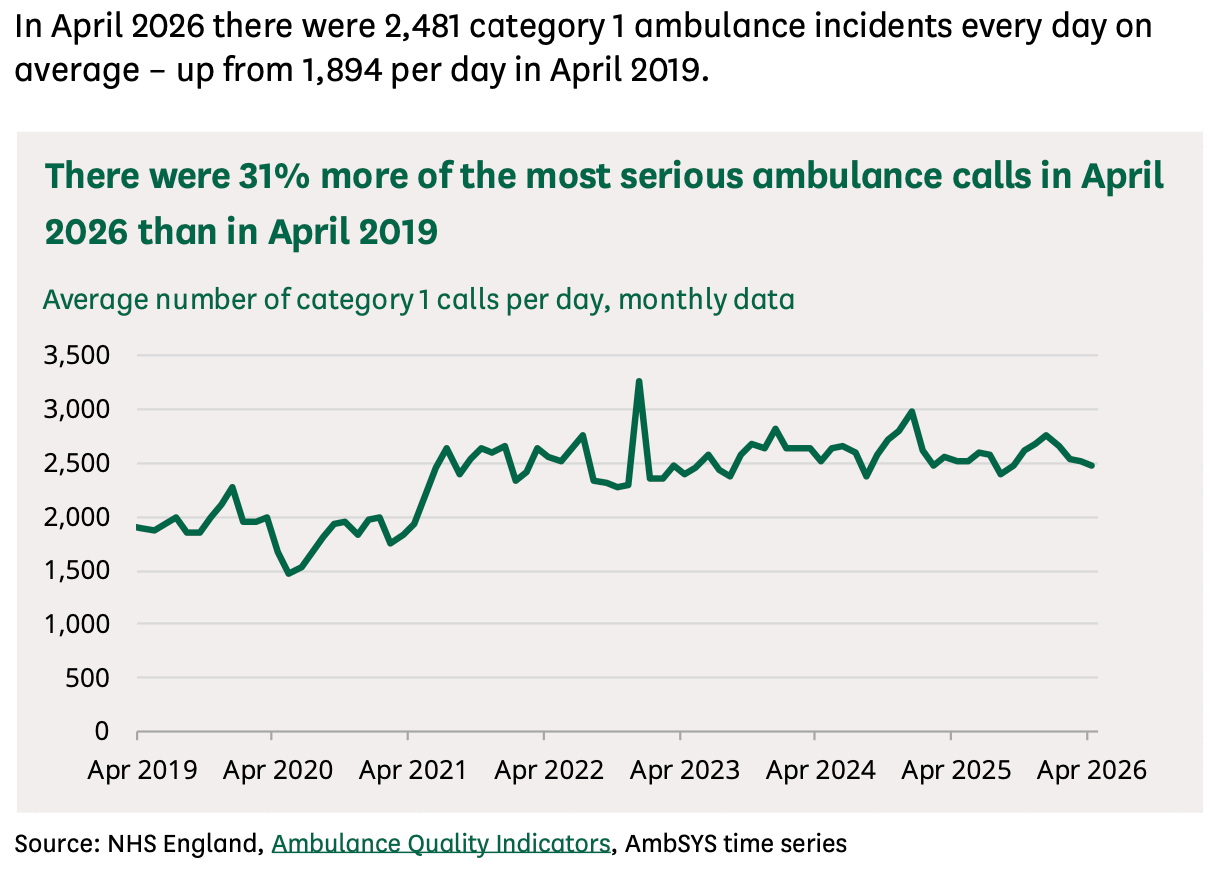
An extra 600 or so serious ambulance calls per day amounts to roughly 200,000 extra per year. Four serious ambulance calls instead of three.
[Dr Patterson] And then… I had an 82-year-old man who only took his vaccine because he wanted to go to America to be screened at the Mayo Clinic… his view was, “You can go to the Mayo Clinic and get everything done in a week which the NHS will take a year to do…” So he got a Moderna vaccine and then within four weeks he was having this strange chest pain... I admitted him [to hospital]… it wasn’t typical of chest pain from a [heart attack]...
And the next day he said to me, “Dean, I want to go home…” He was one of these independent men… a self-made man… didn’t like hospitals. And I said to him, “No, you can’t go home… your troponin has gone up to 8,000.” He said, “No, I feel fine.” And he was adamant, and he was… glaring at me. He was stood up… as tall as me… and he was quite intimidating. And I had to spend the next 45 minutes trying to talk him from going home. And his troponin [see below] sat there… no chest pain… at… between 7,500 and 8,000 for about five days. And that doesn’t happen with [a heart attack]…
And in that week I had about four other patients I diagnosed in the outpatient department with myocarditis… When you vaccinate people in cohorts like this… you get waves and ripples coming through which are associated with each other…
[Doc Malik] Can I just stop you there… You’re a really smart cardiologist… and I hate to interrupt you… Can you please explain what troponin is? Why are you measuring it? What is the normal range…?
[Dr Patterson] Troponin is a protein that’s found inside [heart] cells. It can be released from other areas as well to a lesser degree, but it’s very specific to [heart] tissue and it leaks from damaged tissue or dead tissue… We have… a very, very sensitive test. So if you were to have what we call a heart attack that people in the street would be able to diagnose… clutching [the] chest, sweating… and if you have pain for an hour and you don’t go to the doctor… and you only get to the hospital four hours later… your troponin will go up.
Commonly it’s… [10,000 to] 20,000 if you don’t get medical attention. It really climbs up high. But… [the test] can pick up small… but significant releases [of troponin from the heart muscle] which tell you what’s going on with the patient. So it’s a fantastic test for telling us when you’re getting damage in the heart muscle, from whatever cause that may be... [And] it’s used [everywhere] across the world now.
When you have a normal heart attack, it goes up and comes down in a… standard fashion over the period… [after] your chest pain. It will climb for the first 24-36 hours and then start to come down over the next 24 hours. And assuming that your pain is just one episode, it will go up and come down. It won’t just go up and stay there when you have a heart attack. Whereas if you’ve got inflammation in the muscle [that] is not being resolved, it will stay up as long as the inflammation is present…
[Doc Malik] What is the normal value of troponin…?
[Dr Patterson] …in extremely healthy people, you should have less than 3 as your result… We have a range… between less than 3 and 13, which is considered normal range...
[Anyhow] this [82-year-old] chap… he stayed in hospital [but] he refused to go for any invasive investigations. In any event [though] at that stage I’d accrued [at least] 20… patients where I thought, “Hang on a minute.” [And] it wasn’t just me… my colleague had [also] seen some patients…
And I’ve been raising this issue with the local… risk clinical governance team and things like that… and reporting yellow cards… But the Yellow Card System [which, according to its website, “safeguards medical products quality and efficacy in the United Kingdom”] to my mind hasn’t been… very responsive… I didn’t feel they were taking what I was putting in… seriously… It’s basically drop-down menus and… you use a bit of free text… fill in all the fields… you put a lot of detail in there…
And on a few occasions they sent me a request by email to fill in a Word document, which was basically the same data that I’d already submitted to the database online. [And] I thought, “You’re gaslighting me. I mean, you’re telling me [when] I’ve already sent you this information [that] you want me to be your little skivvy and write a Word document for you?” I don’t have time for that. I was like, “You must be crazy.” It just made me quite angry when I saw that. I thought… the people they’ve got running their systems are clearly not taking this with the seriousness which I felt it should be [taken].
So it’s been a difficult time… because… I think people are not willing to accept [what is happening]… People… take on… the trusted views of the medical establishment and then don’t question it for… up to… a couple of years. It must be quite difficult to turn yourself around and change your mind... I think I wouldn’t find it difficult, but I think there must be some… sort of psychological… rationale why people… when somebody’s trying to raise alarm… cling to the [idea] that this person must be wrong rather than entertaining the [possibility] that maybe they have a point.
I am reminded of the many minority reports of the past, not least in the realm of medicine and health care:
![Minority reports [2026 update and re-issue]](https://substackcdn.com/image/fetch/$s_!tZP0!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fcee3c0f3-bd97-4d95-a31c-e490551a1a4f_822x660.png)
[Dr Patterson] And why would I [raise the alarm if there were no issues]? I’ve got no incentive in this at all. I’m extremely busy. As I said, we run a consultant-only service… there’s no juniors. [And] that’s why I think I get a much finer feeling for the pulse of this. In the NHS, there’s… lots of sub-specialties. [But] I’m a general cardiologist and a physician… so whatever goes on, you get a feeling for it. Whereas in the NHS, I can imagine… if you’re a young person with chest pain, you [might just] get a telephone consultation, or you get a chat to one of the paramedics... They might do an ECG if they come around to your house and [then] say, “No, you don’t need to go to the hospital…”
The influence of Big Pharma
[Doc Malik] Right at the beginning you talked about being in Scotland and witnessing cardiology [the study of the heart] and the influence of Big Pharma and how money was involved… Can you explain… a little bit more…?
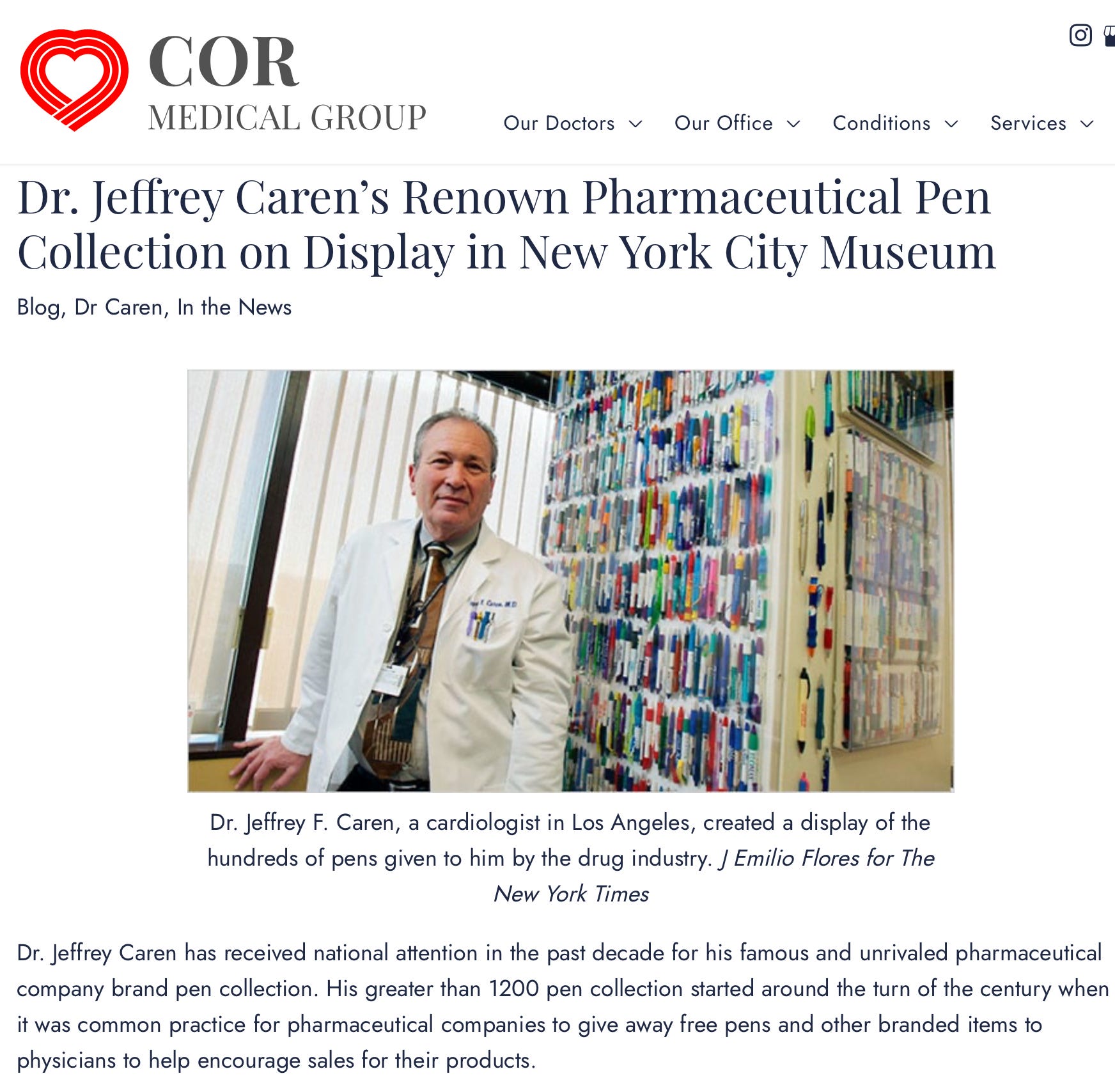
When I was training as a junior doctor I saw the drug reps come… they would host meetings and provide food and drinks and… it’s unbelievable what cheap food can do and how people can be bought with just free donuts and sandwiches… and free pens… and they promote one drug or another… and people would just go and then start prescribing it… it was as simple as that… that kind of simple benign interference. [But in your experience] was it anything more?
I am reminded of the extraordinary pen collection of US cardiologist Dr Jeffery Caren:
[Dr Patterson] [In my experience] it was more about the research grants and the power of drug companies when it comes to doing actual research… and research that’s done in universities, I think, is very much on [drug companies’] terms, and there’s very much... a systematic method of this being done. And I don’t feel that the universities [actually] have… control when they’re doing the research. I think it’s very much [that the universities have] been… almost just a service provider… rather than independent… I feel that the system that is open to abuse… I just think that there is not enough ethical control on the data… independently… with the drug companies being able to veto things. And that was well-established as a reality.
And it was also well-established that drug companies would have guaranteed publications in top journals purely because of the mechanism of the funding. There were all sorts of back doors to getting a publication… One of them was… drug companies would get a publication because the journal knew that it was unofficially a rule that the drug company would order half a million reprints from the journal… and they cost $5 or $10 each. So that’s the back door to getting [pharma] funding [to the journal] for [the] publication. Whereas if you’re just an average Joe trying to get your publication… into a top journal, you’re fighting against that sort of level of financial conflict.
That is a well-established thing which I learned about… Not many people knew… [And] I just found that the university setting was not the place where you get proper blue-sky thought… independent… If you tried to propose some rigorous research, it wouldn’t go anywhere because it was always the drug company’s terms and conditions.
I am reminded of this discussion in this post in relation to The Lancet:

[Doc Malik] I think people need to understand [that, in] these universities and big established departments, doctors chase the kudos… the reputation… the “Look at me… I’m head of cardiology…” “Look, I’m a professor… a senior lecturer.” There’s a lot of prestige attached to these titles… and then you get invited to the lecture circuit… you go to international meetings… you become a bit of a superstar in that little field… Joe Bloggs might not know who you are, but amongst your colleagues and peers you’re a respected authority. So even if you’re not getting a financial backhander… if you’re publishing research and getting promoted and you’ve got papers in distinguished journals… that adds to your reputation. You get the prime trainees working for you… the prime jobs… the lecture circuits. Am I right?
[Dr Patterson] Yes… I think the relationship has led to a situation… that we’ve all come to realise… where so much of what is published is of very dubious quality. And that’s because a lot of these papers are written before the results are through… they just fill in the blanks when the data comes in. And… there is not enough independence in universities... not enough… rigour when it comes to the ethics… Unfortunately pharma has gradually taken [more] control of universities and… I would imagine [it has] got only worse since… I’ve been in Guernsey for 17 years. I think it would be a lot worse [now].
There’s a lot of money now coming through… for example, the mRNA platform. If you look at most tertiary centres [large hospitals that provides specialised medical care] in the UK and across the world, they’ve been planning… launching research projects for not just vaccines, but for all sorts of mRNA technologies to treat cancer and [heart] disease… probably patients with myocarditis, I would imagine… I think there is definitely a huge amount of vested interest...
And unfortunately this is very much on Big Pharma’s terms… because… I don’t feel the tertiary centres are truly independent because they don’t have enough power financially… and the money from Big Pharma isn’t held independently. It should be held in an escrow account, and there should be complete independent editorial oversight from the tertiary centres… and the money should be much more traceable. [At present] money can be flowing in [through] back doors in ways which it shouldn’t, and I think we should avoid that.
Speaking out
[Doc Malik] Going back to Guernsey… [it’s] not the NHS… [but] a different system… you’re not in the same legal structure as England and Wales and Scotland. You’ve got this hybrid system, and you and a group of other doctors offer your services and contract out for the local government… very different from the NHS…
Is it the fact that you were having these thoughts [about Big Pharma] as a trainee… and the fact that you work in Guernsey and have this different system out there… [is that] why you’re more vocal? Because Aseem Malhotra is full-time private… he’s not in the system… that’s why he’s speaking out… It seems like that’s a common theme. You’re independent and you’re not under the thumb of the state regulator or state government. Is that one of the reasons why… you spoke out?
[Dr Patterson] Well, it’s the reason why I was able to speak out. I was put [under] some pressure. I wrote an open letter to the head of the local government [in Guernsey]… where I was openly critical of everything that had happened. I recommended that we follow Sweden and the Great Barrington Declaration. And… I thought [this letter] was pretty good… I’ve got a lot of good feedback from it.
And then subsequent to that… after I’d seen these cases of myocarditis, I wrote an email to the Board of Health and I said, “Look, I would like to know that you are auditing the unintended consequences of your policies.” I listed things like misdiagnosis for cancer, mistreatment for cardiovascular disease, suicide, divorce… people becoming bankrupt… [and] a number of other things I listed there as negatives. And within 48 hours, I was asked by a clinical governance lead to meet him because he said I’d been recommended to have an occupational health assessment because they were worried about me. And I was like, “Well… who made this recommendation?” And he said, “Oh, I can’t tell you.” And so this is a way of putting pressure on you.
I can say other things as well, where I was told… “Why are you seeing this patient? Why are you recommending…” Because this patient [had come] to see me about the vaccination… wanted my opinion… [And the authorities] invited me in on numerous occasions, giving me… this thumb of pressure.
So it’s not been easy… Subsequently… I became more vocal on [social media]… and I’ve then been invited to the management at my partnership and told I’ve broken the social media policy, and that they want… to have a disciplinary process… And I just told them straight, “Look… I’m following GMC guidance… I’m standing for the safety of patients…” And I said, “You should do the same.” I’m not backing down. I’ve reached the point in my life where I am never backing down on this… I won’t back down because I know there’s a problem and… we can’t let this happen…
[Doc Malik] You’re a good medical doctor… you’re abiding by GMC guidelines… you have integrity and you have ethics. And you’re standing up and speaking out for your patients. And in this upside-down clown world you’re getting [persecuted]…
It’s the same script [I’ve seen in other cases]… I got pulled up by the national hospitals management team… the two different hospital groups… same thing… you’re breaching our social media policy guidelines… And I threw it back at them. I’m like, “Policy GMC guidelines 23 and 24… I’m speaking out for my patients. Are you telling me not to?” And then they backed down…
I don’t know what kind of pressure you’ve had, but [from the GMC] it’s just constant pressure… emails… threats for investigations… demands for meetings… And… I’ve… been referred to GMC for apparently being transphobic… because they couldn’t really get me on the covid stuff… And [I’m] just like, “Just back off… because I ain’t stopping. I’m going to keep speaking up for my patients…”
[Dr Patterson] It’s just another massive red flag. When people do this to me, I’m like, “Hmm, okay. I’m learning so much about you people. I’m questioning why I became a partner. Because if you’re all like this, I’m thinking to myself, “Maybe we don’t share the same views. Maybe I need to re-evaluate my compass and actually who I invest my livelihood with.”
I am reminded of this post:

[Dr Patterson] It’s a really tough place to be… but I think I’m slowly… winning people over. You’ve just got to stand up and say it like it is again and again. I feel a bit like an evangelist.
My wife… she’s getting stressed. She said, “Dean, you’re obsessed.” I said, “No, I’m not obsessed. I’m doing what’s right. If I don’t do this, who is going to do it…? Someone has to stand up for the truth.”
I can particularly identify with the second part of that last paragraph.
Fighting for our children’s future
[Dr Patterson] It’s ridiculous... absolutely insane… obscene… as a general physician and cardiologist… all my livelihood I’ve spent… late nights… a lot of people would have packed [it] in. And [then] it comes to… where they do this… and you think I’m going to stand down? You think I’m going to walk away? You think I’m going to keep quiet? It’s not going to happen. It’s never going to happen. Because once you know that… they’ve transgressed and… this is a problem… and they’re not admitting to it… then you know the problem is even bigger than the problem that you’re actually dealing with.
There is a problem behind the problem and we need to fix it… and fix it properly for [our] children… Otherwise, what’s it going to be like for our kids…? I’m 56 and… I’ve got three boys… I work hard now for them… I’ve had my fun, I’ve been around, done a bit of traveling. Yes, I might want to have a nice retirement, but the hard work that I’m putting in… the hard yards… are really for my family. And… you can’t let it go and say, “Oh, it doesn’t matter.” It’s impossible.
[And] it’s not just myocarditis... I’ve seen so many other bizarre things… I saw a 20-year-old chap…. the nurse said, “Come and see this guy… he was admitted by the neurologist… the neurologist didn’t know what was wrong… normal CT… normal MRI… and I went to see him and I looked at him. He was paralysed on the left-hand side of his body… I don’t know if you know what clonus is… the most exaggerated reflex you can have… it’s when your leg starts to jerk heavily. And this guy had… the worst clonus I’ve ever seen… And I looked at him and I was like, “What’s going on with you? You look like you’re having a massive stroke...” And I just got on the phone… I said to the guys in Southampton… “You’ve got to take this kid. It’s seriously something unusual going on here.” And this was in February 2021… I remember this because I’ve never seen anything like it in my life…
Later on that year… I remember the physician who admitted him, because when you admit someone… you’re responsible for when they come back… the patient is yours… [And] I said to her, “What happened to this chap? What was the diagnosis?” She said to me, “Oh, they think it was Lyme’s disease.” So I said, “Lyme’s disease? We don’t have Lyme’s disease here…” I thought… he couldn’t have been traveling very much because we’ve had all this lockdown and stuff…
Anyway, I’m just a naturally inquisitive guy, and I thought, “This sounds really odd.” So I phoned him up and I said to him, “Hi, I’m Dr Patterson… I sent you over to Southampton... Can you tell me what happened?” He said, “Yes… they thought I had Lyme’s disease but then they realised the tests for Lyme’s disease were false positive… Then they diagnosed me with the Guillain–Barré Syndrome…” In layman’s terms… [that] is what we call an ascending paralysis. It starts in your feet and comes up and gradually comes on. And it’s classically with… no reflexes. [But] this chap had clonus, which is the complete opposite… the most severe reflex you can ever have… And he said to me, “Oh, this [is the] Miller-Fisher variant of Guillain-Barre syndrome.”
I was like, “Hmm… I’ve never seen anything like this…” And this was… about the time that this patient of mine at 42 had died. And I said [to the 20-year-old], “Have you had the covid vaccine? Because you’re only 20… you shouldn’t have had it.” And he said, “Yes, I’ve had it.” He had it early. I think someone in his family was a healthcare worker who said he got early access to it.
It’s these things that make a huge difference to your understanding… I feel like I’m seeing the grains of my career… and everything founded upon these things… which people willingly just gloss over. This is absolutely impossible to walk away from. If any clinician had seen a patient like this, you’d remember it… because it is the most severe presentation you would see in a 20-year-old…
Why are so few cardiologists raising the alarm?
[Doc Malik] Dean, how many cardiologists are there in the UK?
[Dr Patterson] I’m not sure, to be fair. I’m not sure… probably a thousand… or maybe two.
[Doc Malik] Why have we not heard from any other cardiologists…? Is it just bad luck in Guernsey…?
[Dr Patterson] I’m at the coalface. We have no juniors. When there’s a problem… something odd happens… you see it. I’ve been here 17 years. I know... the pace of this place…
In big centres and in smaller centres, there is shift-working… you have junior doctors working shifts, coming in, going out… every few months there’s a whole new set of juniors. There’s that effect. [Then] you’ve got the middle grades and… consultants in various different levels and different centres working different shift patterns. In some tertiary centres, some consultants do one shift in a month and a half. So it’s going to be a very delayed signal.
Then in cardiology, you’ve got [dedicated] centres… where if you get chest pain and they think you’re having a heart attack, you go directly… [and] have consideration for a stent. Anyone not fulfilling those criteria will get bounced around between the emergency department, which… is a horror show… or telephone consultations… a popular thing since covid… So you’ve got this perfect storm where the signal is going to be very much dampened down. And that is the problem.
People have also been brainwashed to say that covid causes myocarditis and the vaccines are safe and effective. And they’ve just… said, “Yes, we believe you.” And they’ve become absolutely convinced that they are right based upon that simple, flawed interpretation… a lack of critical thinking. And I think it’s going to be a very difficult time for people to… actually get over this. Because… it’s quite apparent to me that… these vaccines… it’s impossible to say they’re safe and effective… even if they were safe and effective… because the data wasn’t there.
So we had to [look to] real-world assessment of our patients. But we were told that [the vaccine] was safe and effective. [And] anybody that was going to question whether a patient’s admission could be from [a] vaccine side-effect was told not to consider that, which is completely against ethics… completely against any common sense thinking or any normal practice… Can you imagine pre-covid, if we had launched some product with such a short research background and then told people to ignore it. They wouldn’t have… They would never have done it. But it was that complete media propaganda storm that sold everyone into this lie…
[Doc Malik] And I think… they piggy-backed onto the term “vaccine”, which they’ve massaged into the people’s minds [as] being the sacred cow. Because of [Andrew] Wakefield and the scandal, no-one can...
[Dr Patterson] Yes, it was the saviour. It was like a religious thing… “Once we get the vaccine, we’ll be safe.” Once we vaccinate… what [was] it… 15 million people, we’ll stop. You know the story…
There were so many aspects of the covid era that resembled religion:

Several would make for really useful sermon illustrations. But I am yet to hear of them at the church I attend…
[Doc Malik] That’s the problem… they’ve used the sacred cow vaccine… because you can’t question it. If you question a vaccine, you’re a quack and an anti-vaxxer and a dirty idiot. And the funny thing is… this isn’t even a vaccine… it’s gene therapy [or a] gene mis-therapy… It’s a lie on a lie.
[Dr Patterson] Yes… vaccines are given a light-touch regulation compared to drugs… This new type of treatment should, in my view, be given even greater scrutiny than drugs. Instead, it’s been dumbed down into the vaccine slot where they do the basic studies in animals… but when it comes to the humans, the vaccines don’t get any of that assessment, whereas drugs do. So the vaccines get away with it… because all they’re interested in, once they transition to humans, is… they make sure no-one drops dead immediately, which is obviously a big safety signal… They just… want to know about antibodies. If [a vaccine] produces antibodies, they go, “Oh, we’re onto a winner. It’s a vaccine, guys. We’ve got antibody production...” And then they just go into… what they call… long-term safety… where they look at clinical outcomes…
I am reminded of this presentation from US civil rights lawyer Aaron Siri summarising many of the issues in relation to childhood vaccines generally, and particularly the lack of long-term safety data:

Covid, myocarditis and how trials are conducted
[Doc Malik] Moving back to covid, can you tell me… what is the reality of covid and myocarditis…? Does covid cause myocarditis…? Can you shed some light on that?
[Dr Patterson] I think covid is like any other virus in terms of its incidence of myocarditis. I don’t think covid has a specific predilection for myocarditis. I really don’t. I think… if you’ve got a sick patient and have a viral infection or sepsis… myocarditis can be a consequence…
I’ve seen so many people come to me and say, “I went to get my booster and I’ve got a side-effect.” And I said, “Were you feeling well before the booster?” They said, “No… I was breathless, ever since the shot I had before.” And there are so many people who’ve had symptoms [like that]… [And] when you go and get your vaccine, they don’t quiz you. The fact that you arrive is [taken as] “You’ve consented, because you’re here.”
Whereas when you enter… a research project, you get assessed by either a research nurse or a research fellow… a very strict protocol, and they ask question by question, “Have you got any of these things?” So anybody that was coming for their booster who might have been… slightly off… [from] the previous jabs… would get thrown out… And you can see that they… screened 1,800 people to get 800 into the studies… there were… more than twice the number of people… they needed… so there were obviously a lot of people that they didn’t allow to enter the study… [And] that’s odd… because these people were… students and staff at the university… they weren’t people in hospital So, why have these people all been excluded? You’ve always got to look when you see research… [and ask] “Why are the people being excluded…?”
[On a] video I presented, [one] study had a really interesting protocol. They had what we call a screening six-week period where they gave you [a statin to lower your cholesterol] and then they reassessed you. And then they tested your cholesterol and they asked you how you felt. And if you didn’t feel very well on [that statin] or your cholesterol didn’t change, they rejected you from the study. That was called the “screening exercise” [laughs]… there were 6,000 people rejected from their study… and they weren’t able to tell us the screening [results]…
[Doc Malik] Yes… the patients that prove the thing doesn’t work… they just get rid of… politely…
[Dr Patterson] I think they had… maybe 20,000 people in the study, but they had to screen 26,000 people to get the 20,000. So there were 6,000 people that potentially either didn’t tolerate [the statin] or [for whom] didn’t work… which tells you about side-effects and efficacy. And they just ignore that…
I am concerned…. in the last couple of months, I’ve been testing anti-spike antibodies, purely because I’m trying to get a grip. We haven’t got the ability to determine what’s going on in patients. Some people had four or five shots and some people have only had one or two. And we don’t really know how the safety signal works. If you have two, can there be [something] that leads you to having a side effect [several] years later? Or is it only in people that have [had] a fairly recent vaccine… say within the last six months…? When is it safe after the vaccine? When do you feel that your risk is going away? How do we know? We don’t know so many things…
And so I’ve been testing this… you can measure the level of the antibody… [and] it’s been fascinating, because I’ve tested about 30 people who’ve had the vaccine, and 26 of them have got levels of antibody more than the upper limit of the [test]… the [test] can only measure up to 2,500… and 26 out of the 30… it might be more than that… have got levels of antibody above the upper limit...
Now these patients… some of them have had a vaccine two years ago and have no symptoms. Some of them were invited for the booster, and I said, “Well, hang on a minute, I’m not sure about the safety of this.” And they trusted me. So I said, “Well, let’s check your antibodies. They’re about to be boosted.” And the antibodies are more than 2,500... I don’t know how high. We don’t know because the test… stops at 2,500.
Now for comparison, unvaccinated patients… I’ve looked at their results, and they tend to be around 40… 50… maybe up to 100… I’ve not been vaccinated. I’ve had covid. I’ve got antibody levels of 50 to 100. Whereas people that have had… either two jabs or four… and some of them might have had covid… some of them not had covid… why have they got levels of antibodies so high? What is going on? This doesn’t make sense. We were told [the vaccines] don’t work for very long… they don’t have durability…
[Doc Malik] But these are the questions… how long do the spike proteins last for? How long are they made in the body…?
[Dr Patterson] As clinicians… we need to look into this. I don’t want to be alarmist to people, because I think it’s not clear. But my advice to people who have had the vaccine is to understand that you can upset your genes, and the human body is fairly resilient, and you have this thing called the phenotype which is the person you see, the person that grows from [a] baby. The baby is programmed genetically, and what the adult looks like and what the adult suffers with respect to illnesses in their life is down to what you do to those genes. And that’s called the phenotypical expression…. it’s the output from the genetics…
[And] it’s very important to understand that there’s a huge amount that can be done to ensure that you promote the safe expression of your genes and your genetic function. There are some people that have inherited genes from their parents that could cause certain illnesses… and they don’t always get those illnesses. And that’s due to the effect of lifestyle... There may be people out there who’ve got high levels of antibodies who are living… healthy lives… [and have no issues]. It’s very important that we ensure that we don’t stress people. We’ve had too much stress in the last few years, and I think it’s very important to get that message over… that we’re inquiring about this for the right reasons. We don’t want to alarm people. We want to help them
[Doc Malik] Yes… I agree with all of that. We don’t want to be stressing people out. We don’t want to all be doom and gloom… I believe that the human body is very resilient. We are more than just our genes. Hereditary disease is a tiny fraction of illness. Most of it is influenced by epigenetics… by our lifestyle… our environment… stress. So it’s very important to think positively.
Now, I just want to go back to a couple of things… you talked about measuring antibodies… what is the test that you can do…?
[Dr Patterson] It’s the… covid spike antibody test, and it’s measuring the amount of antibody. You can [also] do a test which tells if you’re positive or negative, which is not a numerical result. [But] this specific test will tell you numerically, on a scale, in units per millilitre of blood… how many antibodies you have… the concentration…
[And] we’ve been told that the covid vaccination induces some immune protection, but you require boosters because your immunity wanes. And that would mean that your antibodies should drop after vaccination… they should disappear or become very low. It’s important to understand that… these… antibodies will be produced when you have covid or when you get the vaccine. And… we need to learn how your antibody response is determined when you do get covid after [getting] one or two or three or four vaccines. And then some people have had covid after vaccination and then got a booster. And… quite a few people have had the vaccine who have had covid more than once. And I think there is some sort of immunological interplay there…
[Doc Malik] I don’t know about you, but [now] I just have so many questions… What are these spike proteins doing to the body? How long are they being made for? Where are they going in the body? How long will they last for? You said you can’t measure spike protein. Why can’t we measure it? The body’s meant to be making spike protein…
[Dr Patterson] It’s amazing. We had the PCR test developed so quickly after we discovered this unique virus called covid… rolled out within months. And yet we can’t test… in a commercial sense… for the spike protein. There are some people who have done it in the laboratory and… reading up on that… it does sound like a fairly complicated procedure, but… most blood tests are quite complicated… it’s like a mobile phone… they’re very complicated, but when you commercialise it and start selling in volume it becomes economically viable. You just have to invest in the technology… [and] I think there’s no one wanting to invest in [testing for spike protein]…
For anyone whose health has declined since 2021, and who took the covid injections (and especially the boosters), it is worth at least considering the possibility of covid vaccine injury. I featured some advice from GP David Cartland in this section of November 2024’s Updates post, and I have reproduced it in this footnote1 for reference.
[Dr Patterson] We know that there is so much money riding on… the mRNA technology empire… that it’s extremely difficult for people to be allowed to speak out. You know this… people in the NHS and across the world… have been censored… dismissed… they’ve lost their jobs… even for not taking the vaccine, never mind questioning it. And [I’m] in a unique position… I’m in a partnership where if they dismiss me… it’s a hard blow for the partnership because… you can’t just recruit people into Guernsey… and then you have to have a locum and all that… financially it’s equally hard for them as it is for me. And it wouldn’t go down well because… I think I’m reasonably well-respected amongst my patients… I’m not perfect [but] I’ve always aimed [for] 100%…
The long haul
[Doc Malik] My colleagues tell me… a strange thing is happening. They tell me it’s the vaccine. And I tell them “Why don’t you speak up about it?” And… they say, “No… I’m not going to do that.” They shake their head and rush out of the room. I’ve had three consultants tell me, “You must be kidding… No… I’m not saying anything now.” And that’s desperately sad. What kind of state of affairs are we in now… where doctors are terrified to speak up on behalf of their patients because they’re worried about what’s going to happen to their career and their jobs…?
Do you worry that you… if you carry on talking and speaking up… are going to be made an example of… like Andrew Wakefield…? Because they went for him big time… I’ve had lawyers and journalists tell me that he was made an example of… he was made a scapegoat so that no one would question vaccines… Are you not slightly nervous that they’re going to come for you… they’re going to take your licence away… they’re going to get rid of you… they’re going to discredit you somehow? Are you not even remotely worried about this?
[Dr Patterson] I know the system has to change. I think I’m in a battle. I’m in it for the long haul… for the rest of my life. I don’t expect to see tangible results of my battle personally, but I’m doing this so that my children will inherit something that resembles a respectable system of health. And nothing else matters… at the end of the day… they can chuck me out… go on… do it… I’ve reached the point of realisation… [and they] will just empower me to become [a] bigger voice because I’ll have the freedom to speak, and be the person who I am becoming. [They] will just accelerate me into a place where I can have that personal freedom.
I think there’s [two] sides to this coin. And the people on either side of it need to listen to each other. I think civilisation really needs people to start listening. It’s really important that we do this for societies… for the benefit of the greater good. That’s really, really key to what I’m trying to do. Because there’s bigger things at play here…
[Doc Malik] If you could say anything to your colleagues… all the doctors out there, what would it be…?
[Dr Patterson] If I were to sit down and have a chat… I would say to them… “Why are you in medicine? What are you actually in this for…?”
Everything hinges on that. Because… believe it or not, I think a lot of doctors are completely lost. I think they’re in medicine for the wrong reasons. And once you know who you’re talking to… a clinician [or] a businessman… your response to them will be guided by that… it’s very difficult to have one answer…
If they aren’t engaging, I do what I do every day with them. I say to them, “Look, there is a problem. I think that I am an intelligent, wise clinician. I listen to my patients. I have my patients’ best interests and… your best interests at heart. I am not the type of person to waste anyone’s time on frivolous tasks… I am the type of guy who calls a spade a spade… [and] I’ve got 101 other things… I could be doing… but I can’t let this slide…”
And this is the sort of doctor that the GMC suspends…
In more ways than one, this stirring instrumental track seems an appropriate way to end this post. Its name is Heart of Courage. It is by Two Steps from Hell. And it is taken from the album Legend:
It would be a fitting tribute to anyone who has spoken out in the context of the events of the past few years, not least those in the medical profession.
Related:


And also:




![[IV] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/$s_!70T3!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fcd3f9ba8-d8f9-422d-924a-1e07a5103af6_874x882.png)


Dear Church Leaders (and everyone else) homepage
Some posts, including a version of this one, can also be found on Unexpected Turns
Revealing Faith: Seeing and believing the revelation of God
The Big Reveal: Christianity carefully considered as the solution to a problem
Dr Cartland’s original post was not available at the time of writing, owing to his X account having been suspended, but it stated:
If you suspect a jab injury and are being gaslit by your doctor please DEMAND: autoantibody and Vasculitis screen! They won’t want to because they know what it will show! ANA ANCA et al and inflammatory markers eg CRP/ESR as well as ddimer!
I did a 19 patient small study early 2024 and every single jab injury was ANA positive to varying titres.
Jargon buster:
Autoantibodies are specific antibodies produced by the immune system that target the body’s own cells and tissues, leading to inflammation and potential dysfunction. They are commonly found in autoimmune diseases and play a significant role in diagnosis.
Vasculitis is a group of conditions that cause inflammation of the blood vessels, which can affect different organs and cause various symptoms.
ANA, ANCA, CRP/ESR and D-Dimer are blood tests:
ANA stands for anti-nuclear antibodies, which are relatively non-specific markers of autoimmune disease, particularly connective tissue diseases.
ANCA stands for anti-neutrophil cytoplasm antibodies, which are autoantibodies that target a type of human white blood cell called neutrophils, which are important in health for fighting infection partly through the release of toxic substances that destroy bacteria.
CRP and ESR are tests that can be used to check the levels of inflammation in the body. CRP stands for C reactive protein, whose concentration rises in response to many pathological conditions, including infection, tissue injury, response to surgery, inflammatory disorders, and associated diseases. ESR (not to be confused with Electronic Staff Record) stands for erythrocyte sedimentation rate.
A D-dimer test detects some of the breakdown products of clotting in blood.