


The measure of society is how it treats the weakest members
Scottish Covid Inquiry evidence from the Disability Charities Consortium
Dear Church Leaders (and everyone else)
This post features testimony from the Disability Charities Consortium (DCC) to the Scottish Covid Inquiry which I first featured here:

And then also in this update.
But before considering what was said, here is a reminder of three pieces of important context:
Three pieces of important context
The words of Chris Whitty in March 2020
The Chief Medical Officer for England, when taking questions from a UK Members of Parliament in early March 2020, stated that:
It is clear that the risk [of covid] is very heavily weighted towards older people
Here is the relevant clip:

The ONS data from early 2020
Below are snapshots of data from the UK Office for National Statistics which anyone can easily look up and check:

In February 2020, when we were told that covid was circulating, there were fewer deaths registered than in any of the previous five years. And 2020 was a Leap Year!
And in March 2020, even with the chaos that ensued following the announcement of lockdown on 23rd, there were still fewer deaths than in the same month in 2018.
Links to the data can be found in this post:

And the table below features a more detailed summary:

According to official UK government data, until Britain was ordered into panic mode on 23rd March deaths were at normal levels for the time of year
The Disability Charities Consortium (DCC)
According to this website:
The Disability Charities Consortium (DCC) brings together leaders from the UK’s leading not-for-profit disability organisations to work with the Government to make sure disabled people’s experiences are reflected in UK policy making.
The DCC members are:
DCC closing statement to the Scottish Covid Inquiry
The closing statement from Jamie Burton KC for the DCC can be found here (1:47-7:55, transcript below):

[Covid-era UK Health Secretary] Matt Hancock’s evidence… caused very significant alarm. The DCC is not aware of any evidence to support his contention that covid-19 was intrinsically more aggressive against people living with disabilities.
Did he really think the virus — or does he really think that the virus — knows if somebody has a learning disability? Or knows if they have a hearing or visual impairment? If Mr Hancock really was of this view, it is not surprising that, under his leadership, little was done to address disparities.
It is clear that there was was misuse of DNACPRs [Do Not Attempt Cardiopulmonary Resuscitation orders] which affected disabled people adversely. This was not surprising. We know it happened before the pandemic. We also know that disablism, conscious or otherwise, was and remains a very real phenomenon in society.
But on this there appears to have been a profound state of national cognitive dissonance. Every witness was unanimous that blanket policies are outrageous, but yet… research showed that 78% of deaths of learning disabled people in the first wave were in relation to cases where DNAPCR attached to the individual concerned.
Here is a table featuring the official ONS data for registered weekly deaths in England and Wales in the six weeks before and the six weeks after the introduction of the “covid measures”:
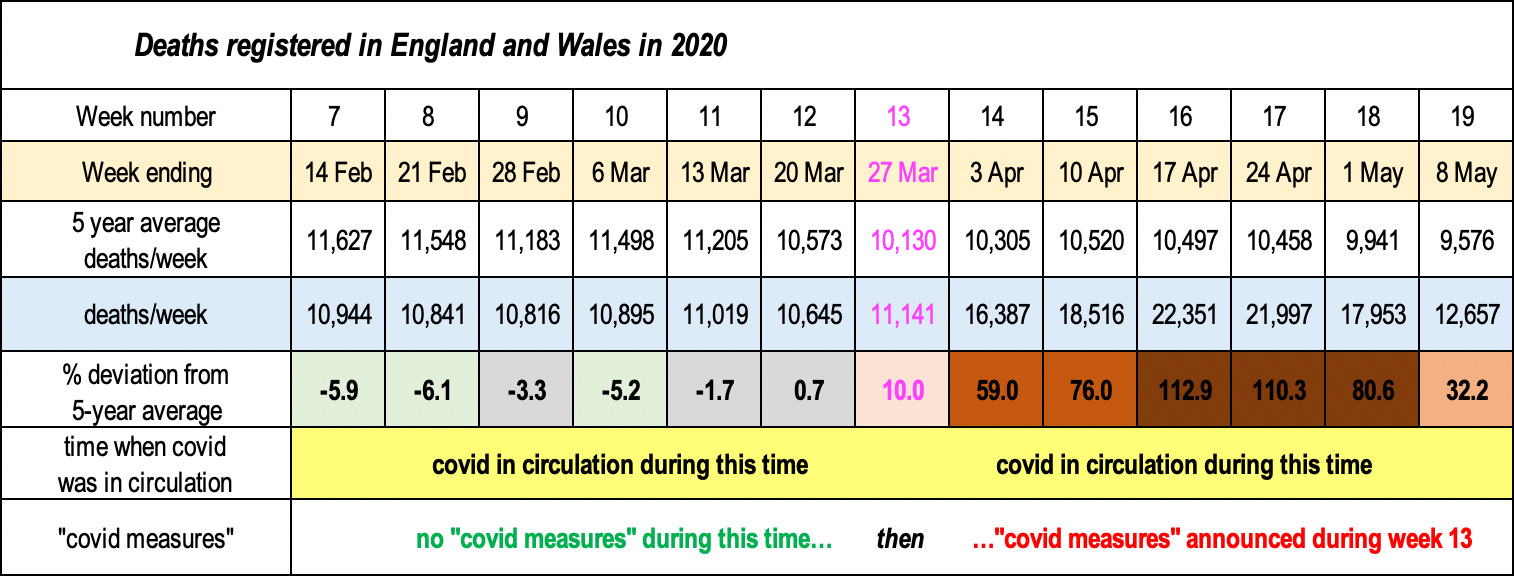
To reiterate, the inconvenient truth is that the death rate increased only after the first lockdown began and the “covid response” began. When people panicked. When people were terrified by their governments. When people were told, “Don’t come into hospital if you can help it.”
I couldn’t easily find the historic data for average deaths/week in Scotland, but, according to data here, the pattern of Scottish deaths in 2020 is similar to that in England and Wales:

NB in an average year there would be around 10% fewer deaths in April compared with February (cf. the average deaths/week data for England and Wales above).
As in England and Wales, the death rate in Scotland increased only after the country was ordered into panic mode.
In addition to this, as the CQC [Care Quality Commission] so powerfully described in their report, DNACPRs are often seen as a proxy for do not treat notices, and confusion reigns about how and for how long a DNACPR should be applied
On the 20th March 2020, NICE [the UK National Institute for Health and Care Excellence] published rapid covid-19 guidelines on critical care in adults, which advised that all adults — not just those over 65 — should be assessed for frailty using the clinical frailty scale.
Why did they do this, given that, in the words of England’s Chief Medical Officer, it was “clear that the risk [of covid] is very heavily weighted towards older people”?
As the inquiry experts explained, “the nature of the indicators used may have overestimated the risk of a poor outcome in people with stable conditions such as cerebral palsy or learning disability. A higher clinical frailty score [CFS] may reflect their stable disability and not, as intended, their overall ability to receive treatment.”
CQC confirmed in its interim report that the use of the CFS was interpreted by some as meaning that disabled people who were not frail, but needed assistance, would be denied access to critical care. It was only after the persistent intervention of Mencap and the National Autistic Society that NICE revised the guidance to make it clear that the CFS should not be used for younger people or those with learning or stable long-term disabilities.
However, while the changes were widely communicated, Mencap concluded in its report, My Health, My Life, that the original guidance had ongoing damaging consequences, as in “GPs had sent letters to care settings implying that people with learning disabilities would not be treated if they went to hospital, and [that] advanced decisions including DNACPR orders should be made.” As Jackie O’Sullivan put it, “the genie was out of the bottle, and it was very hard to put it back in.”
As pathologist Dr Clare Craig points out succinctly:
People with learning disabilities were denied healthcare and died at a far higher rate
If you withdraw healthcare you get excess mortality
Those excess deaths were then weaponised to push for more restrictions
Mortality rates… what we know and, importantly, what we don’t know. The DCC started its submissions here, and it’s appropriate to finish here.
All the evidence shows that, even when controlled for age, socio- and economic status, co-morbidities, health and vaccine status etc, there were still very significant disparities in mortality for disabled people when compared with the general population.
The government was aware of this from late June 2020, but it did not feature in the Public Health England reports. Indeed it only became central to government thoughts very late in 2020, after the Equality Hub was set up. And even then, most of its recommendations including around access to healthcare, communications and consultation, were not followed. And sadly, as we all know, the rate of disparities and mortality in the “first wave” were then replicated in the “second wave”. You might think there is a lesson right there…
The harsh reality is that, despite the… legal obligations to take steps to protect disabled people from disadvantage, precious little was done. Shielding was entirely focused on clinical vulnerability, whilst those with living Down’s Syndrome were added to shielded persons list. A policy predicated only on medical conditions, rather than a wider social model of vulnerability or disability, always risked overlooking entire categories of disabled people, leaving them without a mechanism to ameliorate risks effectively and quickly.
I am reminded of these words of Thomas Jefferson:
The measure of society is how it treats the weakest members
It is perhaps somewhat surprising, given what has gone before, that Burton adds:
…beyond that statement of principle, the DCC is hard-pressed to advocate what should be done or might be done in a future pandemic, because even now, some four years later, we do not know what caused the disparities.
It’s worth reiterating here that Biologyphenom/Dave, the author of the Substack featuring the above video and others like it, still cannot post on X (formerly Twitter).
It’s also notable how little coverage the Scottish Covid Inquiry has received in the mainstream media.
Biologyphenom/Dave’s take on the above video can be found here. He concludes with this recent post from UK barrister Francis Hoar in response to Matt Hancock’s delight at the recent vote on Assisted Dying:

Again, the measure of society is how it treats the weakest members.
I suspect that Francis Hoar is confident that the covid-era Health Secretary won’t be taking legal action here.
On the subject of delight, it’s worth watching this short clip of Hancock being interviewed at the time of the rollout of the first covid injections.

Genuine tears of joy? Or Duper’s Delight?

Dear Church Leaders most-read articles
Some posts, including a version of this one, can also be found on Unexpected Turns
The Big Reveal: Christianity carefully considered